Corrective osteotomy according to Ilizarov. Types of corrective osteotomy, rehabilitation after surgery
Osteotomy is a surgical manipulation, the essence of which is to create an “artificial fracture”. During the operation, the bone is cut into two parts. After that, the bone fragments are displaced in the desired direction and fixed in an anatomically favorable position.
Osteotomy of the tibia.
Indications for surgery
In clinical practice, osteotomies are most often used to correct axial and torsional deformities of the lower extremities. Such operations are done with hip dysplasia, leg length discrepancy, flat feet, valgus deformity of the foot, curvature of the upper limbs and spine. During surgical interventions, surgeons can cut long tubular bones, vertebrae, pelvic bones or feet.

The main purpose of osteotomy is to correct the distribution of load on the joints. With the help of surgical intervention, doctors can restore the normal functional state of the joints or “unload” their damaged parts.
Benefits of Corrective Osteotomy
During the intervention, surgeons separate the bone into parts using a saw, drill or chisel. They perform all manipulations in accordance with a clear preoperative plan. During preparation for surgery, doctors create an optimal scheme for correcting existing defects. Naturally, this tactic allows you to achieve good functional results.
Video in English, but very informative:
During an osteotomy, surgeons do not touch healthy joints. This allows you to save their functions and avoid complications associated with the opening of the synovial cavity. If the joint is damaged, bone repositioning will help slow down its destruction. For example, osteotomy can delay the development of deforming arthrosis, delay joint surgery for 10-15 years.
In the presence of severe osteoarthritis or weakness of the ligamentous apparatus, one osteotomy may not be enough. Therefore, to achieve the desired effect, doctors supplement it with reconstructive operations on the ligaments, arthrodesis or other manipulations.
For example, in case of flat feet, corrective osteotomy of the foot is often combined with plasty of the long plantar ligament and arthrodesis of the subtalar joint.
Preparing for the operation
During preoperative preparation, doctors examine the patient and select the optimal treatment plan for him. After that, the specialists must coordinate it with the patient himself. Before surgery, each person undergoes a full examination.
The list of necessary analyzes and studies:
- general analysis of blood and urine;
- determination of blood group, Rh factor;
- blood tests for RW and HbAg;
- coagulogram;
- blood chemistry;
- radiography in 2 projections;
- magnetic resonance imaging (MRI) of the affected segment;
- consultations of a neuropathologist, cardiologist, endocrinologist, allergist and other necessary specialists.

The more thorough the examination, the lower the risk of complications.
While waiting for surgery, doctors advise patients to perform special exercises. They help to stretch and strengthen the muscles, which makes it possible to avoid the appearance of contractures in the postoperative period.
Some doctors refuse to operate on patients with severe obesity. The reason is a high intraoperative risk, difficulties in rehabilitation and a high likelihood of complications. Such patients are usually operated on after they lose weight.
The patient is admitted to the hospital 1 day before the operation. There he communicates with the attending physician, signs an informed consent for anesthesia and surgical intervention. After that, the patient is prescribed the necessary drugs, which he takes under the supervision of the medical staff.
On the evening before the operation, the person is forbidden to eat. In the morning he is asked to remove all jewelry. Immediately before surgery, the patient is dressed in sterile clothing and taken to the operating room.
Operation progress
Osteotomy can be performed under general or local regional anesthesia. The choice of method of anesthesia depends on the volume of surgical intervention, the general health of the person and some other factors.
The operation begins with a layer-by-layer dissection of the soft tissues. Having gained access to the desired bone, the surgeon cuts it. After that, he fixes the bone fragments using external (Ilizarov apparatus) or internal fixation systems (bone plates, screws). Before suturing the wound, doctors often conduct a control X-ray examination. It is necessary to confirm the correct fixation of the bone.The operation lasts from 60 to 120 minutes.
Rehabilitation after corrective osteotomy
After surgery, a person stays in the hospital for 3-7 days. In the postoperative period, he is regularly treated with a wound, given painkillers, antibiotic prophylaxis and prevention of thromboembolic complications. Also, the medical staff ensures that the patient begins to get out of bed as early as possible.
After discharge from the hospital, the patient goes home. There he continues to take the drugs prescribed by the doctor. He moves with the help of crutches. The sutures are removed for the patient 10-14 days after the operation. After an osteotomy, a person must undergo a full rehabilitation.

Most common complications
Sawing bones is a serious intervention, the implementation of which is associated with considerable risk. Undesirable complications may develop during the manipulation or already in the recovery period. Many of them are difficult to treat.
Table 1. Possible complications
| Causes | Treatment and consequences | |
| Nonunion of bones | Smoking, poor blood supply to the bone, osteoporosis, severe comorbidities | In case of nonunion, the patient needs a second operation and subsequent long-term rehabilitation |
| Vicious union | Improper fixation of bone fragments during surgery | It is possible to eliminate the defect only with the help of one more operation. |
| Violation of the functions of nearby joints | Incorrect rehabilitation or its complete absence | In most cases, joint function can be restored with the help of physiotherapy exercises. |
| compartment syndrome | Compression of muscles with a hemostatic tourniquet during surgical procedures | Pathology is treated conservatively with the help of certain pharmaceuticals. In severe cases, the patient undergoes surgery - fasciotomy |
| Nerve damage | Inattention of the surgeon or "non-standard" location of the nerve in a particular patient | It is impossible to restore the integrity and function of damaged nerves |
| Infectious complications | Infection during surgery or non-compliance with the rules for caring for a postoperative wound | They are treated with antibiotics. In severe cases, the patient may require revision surgery. |
| Thromboembolic complications | Inadequate prescription of anticoagulants, refusal to wear compression stockings, late mobilization | High doses of anticoagulants and antiplatelet agents are used to treat thrombosis. |
Possible Alternatives
Unfortunately, many diseases can be cured only with corrective osteotomy. This applies to congenital hip dysplasia, O- and X-shaped deformation of the lower extremities, severe kyphosis, lordosis, scoliosis. But in the treatment of flat feet, valgus deformity of the foot, osteotomy can be replaced by other types of interventions. The only problem is that they are likely to be less effective.

Osteotomy is the most effective method of surgical treatment of many diseases of the musculoskeletal system.
Corrective osteotomy of the knee joint is a surgical intervention aimed at eliminating the deformity of the bone tissue. When planning such an operation, one should prepare for the artificial breaking of a small section of the bone in order to correct the malunion. There are different methods of osteotomy, differing in the level of complexity depending on the presence or absence of comorbidities and the general condition of the patient.
Indications and contraindications
Osteotomy of the knee is most often performed for degradation of cartilage and parts of the joints of the knee, when it is necessary to preserve healthy tissues.
Contraindications for surgery:
- rheumatoid arthritis;
- local and general infectious diseases;
- diseases of the veins and vessels of the legs;
- heart and lung diseases in the stage of decompensation;
- kidney and liver failure;
- obesity or dystrophy;
- diabetes;
- increased bone fragility.
People who do not fall into the 40-60 age category may be denied surgery due to a low chance of a positive result or the possibility of a more benign treatment.
Correction of the knee joint with an osteotomy is recommended for patients who meet the following characteristics:
- mild to moderate arthritis that only affects one knee
- middle age category;
- optimal weight;
- high mobility of the knee joint: the ability to straighten - bend at least 90 degrees;
- the presence of pain caused by arthritis and manifested only during the period of activity or prolonged standing;
- consent to long-term rehabilitation;
- consent to walk with crutches for 6-8 weeks after surgery.
If the operation is carried out correctly, the positive result will remain for a long time.
Preparing for the operation

MRI of the knee
Prior to osteotomy, confirmation of the diagnosis and determination of the amount of bone tissue to be removed is required. Required research:
- radiography;
- MRI, which uses special magnetic waves to create an image of the structure inside the knees;
A comprehensive examination allows you to understand how high the level of effectiveness of the planned procedure will be.
Before performing an osteotomy, it is recommended to consult a doctor regarding the medications used. You may need to temporarily stop taking certain medications, such as anti-inflammatory and blood thinners, for about a week. This measure increases the effectiveness of surgical intervention.
The operation is done exclusively on an empty stomach, therefore, at least 8 hours in advance, it is necessary to refuse meals, and 3 hours before drinks.
Features of knee surgery
The joints should be corrected until the disease has become more severe and has not led to the loss of the patient's ability to work. With advanced pathologies, arthroplasty is recommended, which involves replacing the affected joint or part of it.
The main task of osteotomy is to normalize the ratios of the surfaces of the knee joints, improve blood circulation in bone tissues. It is possible to remove the load from the affected area, which is subsequently transferred to a healthy limb for full functionality. Stagnation of blood in nearby tissues is prevented, as a result of which the risks of destruction of the cartilaginous tissue of the knees are eliminated.

Result of corrective knee osteotomy
The result of corrective osteotomy depends on the correct calculation of the deformity angle and further surgical correction. To prevent relapse, it is recommended to take 3-4 healthy degrees. Doctors use imaging technology to measure the part of the bone that needs to be removed. Careful control increases the effectiveness of the event.
An incision is made in the skin, and thin wires are placed in the knee to facilitate the removal of the bone. The doctor carefully removes part of the knee joint at a certain angle. The remaining parts are fastened with special medical screws. At the end of the procedure, the tissues are sutured in layers and treated with antiseptics.
Corrective osteotomy of the knee usually takes 1-3 hours, after the operation it is necessary to stay in the hospital for 2-3 days. In some cases, the doctor extends the length of stay in the hospital if he sees complications.
Features of rehabilitation
After corrective osteotomy of the knee joint, rehabilitation is mandatory for the full restoration of knee functions. The set of measures includes:
- Taking painkillers.
- Cold compresses for 15-20 minutes four times a day.
- During rest, the position of the operated leg is higher than the body to eliminate swelling, improve blood circulation and lymph outflow.
- Caring for sutures to prevent inflammation, keeping them clean and dry.
- Use of crutches or walkers initially. The timing of the use of aids is determined by the doctor.
It is necessary to develop a knee after an osteotomy under the supervision of a physiotherapist after 6-8 weeks. The therapy is based on the gradual expansion of the range of motion and includes strength training.
Osteotomy is a surgical operation used in cases where it is necessary to eliminate a defect in the bone tissue. Most often, the procedure is performed to restore the bone after its deformative damage.
Various segments can be operated on, including the bones of the legs and face. Osteotomy is possible only in a hospital, it is not done in clinics. Unfortunately, there is a risk of postoperative complications, especially if serious mistakes were made during the rehabilitation period.
The operation can be complex (in the treatment of large leg bones, for example) and simple (mini-osteotomy). The risk of postoperative complications is higher in case of complex technique.
1 What is an osteotomy: a general description of the operation
Nowadays, almost any problem associated with deformative lesions of bones and joints can be solved without problems. It is for the solution of such problems that osteotomy is used.
The procedure is designed to eliminate bone defects and the consequences of tissue deformation. With the help of the operation, it is possible to restore the functions of the musculoskeletal system, including by means of an artificial fracture.
A patient can deliberately break a limb at the level where the deformity is localized. This technique is often used for congenital or acquired pathologies (for example, an incorrectly fused fracture).
With its description and method of implementation, osteotomy can scare away most patients. In fact, everything is not as scary as it might seem: the patient does not feel anything during the operation (except for moderate discomfort associated with the work of receptors that fix mechanical stress).
The procedure has two types of conduction: through a small incision on the skin or by making several holes in the skin. This technique is used for both children and adult patients of different age groups.
1.1 What is carried out?
The procedure is applicable to the following groups of bones and joints:
- lower and upper jaw;
- pelvic bones, hip joints;
- lower leg bones, knee joint, metatarsal bone;
- elbow joints, bones of the upper extremities, including fingers and radius bones;
- it is possible to treat the femur (a rather complicated procedure that has risks of postoperative complications).
It is important to understand that each group of bones uses its own nuances of surgical intervention. In addition, different techniques can be used even for the same group of bones, but with different diseases.
For example, the femur can be treated using a corrective and restorative osteotomy method. The first option is suitable in cases where there is an incorrectly fused fracture. The second option is preferable for hip subluxation.
The final choice of technique remains with the attending physician. It is done after a series of diagnostic procedures.
1.2 Indications for carrying out
There are quite a lot of indications for osteotomy, because in addition to general diseases (which can affect different joints and bones), there are also specific ones that occur only in a certain group.

Osteotomy is performed for the following pathologies:
- Incorrectly fused fracture of one or another group of bones (in this case, it is possible to carry out an artificial fracture with subsequent normal healing of the bone).
- Ankylosis of a joint in a vicious position.
- Coxarthrosis
- Valgus deformity.
- Consequences of rickets in the form of curvature (deformation) of the bones.
- Traumatic deformities.
- Shortening or pathological lengthening of the bone.
- Dislocations and subluxations of bones or joints.
- Birth defects and anomalies in the structure of certain bones.
- Varus deformity.
- False joint of the femoral neck.
Often, the operation is performed with various subspecies of arthritis (for example, with psoriatic arthritis). The fact is that arthritis can lead to deformities of the joint or bones. As a rule, this happens only in the most advanced cases, when the disease proceeds for a long time.
The specificity of the procedure is the treatment of deformative lesions as a result of injuries or complications of bones, but not joints. Treatment of complications of various types of arthritis is only an auxiliary function of osteotomy, which is not used constantly.
1.3 Contraindications
There are a fairly large number of contraindications to conduct. They cannot be ignored, because in this case the situation can be aggravated up to disability.
Osteotomy should not be performed in the following cases:
- during the period of acute onset or exacerbation of rheumatoid arthritis;
- third degree patellofemoral subspecies of arthrosis;
- obesity in a patient of 2-3 degrees (relative contraindication, in some cases ignored with the permission of the attending physician);
- the presence of osteoporosis;
- violations of the regenerative functions of the body, in particular - local (in terms of bone tissue regeneration);
- infectious pathologies of bone tissue (for example, syphilis or bone tuberculosis) - active or transferred in the recent past;
- arthrotic lesions (degenerative-dystrophic), localized in the collateral parts of the joints.

In addition, it is impossible to perform an operation with a general weakness of the patient, exhaustion, cachexia, fever (even with a minimally elevated temperature). The operation is also prohibited if a clear diagnosis is not established: for example, there are deformative lesions of the bone, but it is not known what caused them. First, a full diagnosis is made - then a decision is made on the operation.
2 Types of osteotomy
The operation has two types of conduct: closed and open way.
In a closed procedure, surgery is performed through a small (endoscopic) incision in the skin. The size of the incision usually does not exceed 2 centimeters. During a closed osteotomy, the doctor literally blindly crosses the bones using a special chisel. This is a difficult and dangerous technique, since the wrong actions of a specialist can lead to a number of serious complications.
Open osteotomy is used much more often, including because of the lower risk of serious complications. Here, the doctor does not work blindly: there is the possibility of a full visualization of the operated tissues. The incision on the skin for this technique is much larger, and is up to 12 centimeters in length.
Also osteotomy is divided into several subtypes:
- Linear subtype (transverse or oblique). The diseased bone is incised in such a way that it is then aligned with the graft (plates). In dental implantology, intercortical osteotomy is performed to eliminate jaw defects.
- Wedge-shaped subtype (akin, Akin). During the procedure, the patient is removed part of the bone tissue, due to which the remaining intact bone is subsequently aligned.
- Z-shaped subtype. Used to treat hallux valgus deformity of the big toe. During the procedure, the doctor removes the overgrown tissue.
- Angular subtype. Bone tissues are carefully cut at certain angles on both sides, due to which it is possible to put them in the required position.
3 How is the operation carried out?
There is no universal method for performing osteotomy: each case (disease) uses its own technique.
For example, during corrective surgery on the pelvic bones, the ilium is dissected in the area above the acetabulum. Next, the pelvic joint is displaced with the creation of an artificial "shield" over the articular head. The procedure is performed under endotracheal anesthesia (the safest option in this case).

Surgery of the knee joints is usually performed for the treatment of deforming arthrosis. Produce the intersection of the tibia, which leads to improved metabolism in the articular tissue by eliminating the stagnation of venous circulation.
The feet are usually treated for hallux valgus. To do this, the doctor makes an incision at the end of the bone adjacent to the big toe, followed by placing it closer to the inside of the foot. As a result, it is possible to eliminate the displacement, but sometimes it is necessary to remove part of the overgrown bone tissue.
Sometimes doctors go to some tricks when operating on non-specific cases of diseases. That is, right in the course of the operation, the standard tactics of actions can change. As a rule, this only has the best effect on the patient's recovery.
Whatever specific procedure is performed, there is always a non-zero chance of complications after the operation. Often, complications are caused by an incorrectly conducted rehabilitation stage.
3.1 Where is it held and how much does it cost?
Such complex surgical procedures are carried out only in large public hospitals or private clinics. It is advisable to contact specialized medical centers dealing exclusively with diseases of the musculoskeletal system.
The cost depends on the type of operation. For example, a corrective osteotomy costs around 50,000 rubles. The average cost of the procedure, regardless of its type, ranges from 60-65 thousand rubles.
3.2 Ligation after osteotomy (video)
3.3 Rehabilitation after osteotomy
Restoration of the function of the operated bone is at least 50% of the success of the entire treatment.
It is important to understand that in most cases, the bone will no longer be functionally the same as it was before the disease and surgery. However, such a restoration of the functionality is possible that there will not be much difference (according to sensations).
How exactly rehabilitation after osteotomy should be carried out depends on which particular method of operation was performed and on which area.
There are general rules:
- In the first time after the procedure, complete rest of the area that was operated on is required. There should not be any load, even minimal.
- Later, the patient is prescribed minimal physical activity to restore bone functionality. A dosed load triggers the acceleration of the regeneration of the operated tissues. The decision on when and how to load the operated part of the body should be made only by the attending physician.
- Medical corsets, orthopedic insoles and other instruments can be used to reduce the load on the bones.
- Medications (anti-inflammatory, regenerative) must be prescribed. Pain relievers and muscle relaxants may be used as needed.
Recovery after an osteotomy can take several months. It is very important to follow all the doctor's prescriptions: improper rehabilitation can not only ruin the effect of the treatment, but also make it worse than it was before the operation.
3258 0
Modern medicine has reached a new level, and now surgical operations to eliminate a defect or disease of the bone no longer lead to such dangerous consequences than several decades ago.
One of the most popular procedures today is osteotomy.
This operation can significantly improve the life of a sick person, so specialists perform it without any fear.
What is the essence of the operation?
Osteotomy is a surgical intervention, the purpose of which is to eliminate a defect in the form of bone deformity, as well as to significantly improve the functions of the musculoskeletal system through an artificial fracture.
The operation at first glance looks rather scary, but according to its results, it is much easier for a person to stand if the procedures were carried out on his feet, or to independently perform simple actions and movements with his hands, in case of surgical intervention on the arm.
The operation is carried out in several ways: by incision of the skin or by making holes.
Fastening of broken bones is carried out using plates, screws, knitting needles and other devices.
Plaster bandages are practically not used, since this is fraught with bone displacement and repeated surgical intervention.
Varieties of intervention
As already mentioned above, the operation can be carried out by incision or punctures, as a result of which the osteotomy is divided into open and closed types.
The closed type of intervention is used extremely rarely.
Osteotomy, depending on the intended purpose, is divided into:
- Corrective surgery- It is used due to an incorrectly fused bone after a fracture.
- Derotational operation- is carried out in order to save a person from pathological rotation of the bone.
- Lengthening or shortening of limbs– sometimes has a cosmetic connotation.
- Surgery to improve support function.
Each type has its own characteristics and reasons for holding.
Sometimes bone fractures are cosmetic reasons. For example, in order to carry out a cosmetic surgery to lengthen the legs, osteotomy is used - artificially break bones for their further lengthening.
Corrective surgery
The presented type of osteotomy is used every time when there is a significant deformation of the bones in the human body.
For example, this type of surgical intervention is used in the following cases: 
- improperly fused bone after a fracture;
- the presence of ankylosis of the joint in a vicious position;
- the presence of bone curvature due to rickets and in other situations.
Corrective osteotomy is sometimes performed by lengthening or shortening the bone, if such actions will lead to a positive result and significant relief to the person.
The operation is carried out in three ways:
- Linear with bone graft- the bone is incised in order to align it through the introduction of a bone graft.
- Wedge-shaped with removal of the bone wedge- a part is removed from the bone to align it.
- corner– the bone is cut at an angle on both sides and is set in the correct position due to the necessary correction.
In most cases, corrective osteotomy is used after bone malunion due to a fracture. The operation is performed under general anesthesia and takes a long recovery.
Limb lengthening
Limb lengthening is the most common operation where an oblique osteotomy is used with skeletal traction applied to the distal end.
Such an operation can increase the operated bone by 2-7 cm.
The main condition is the selection of the correct size of the load. The presented method helps not only to "align the curved" bone, but also to significantly increase its length.
When using compression-distraction devices, it is possible to achieve the result of an increase in the length of the bone by almost 20 cm.
This method helps to increase the limb per day by 1 mm, while the mobility and function of the joints are preserved.
Derotational operation
It is often used after dislocations. If the plaster or tight bandage is applied incorrectly, a kind of reversal of the bone relative to the joint occurs.
Such “contact” causes pain and can lead to dysfunction of the joints - a person cannot do simple actions with his hand, in case of damage to the lower extremities, the patient cannot move.
Derotational osteotomy involves cutting the bone in the transverse direction. Next, the central part of the bone is turned in the required direction at a certain angle of turn.
All participating bone fragments are fixed until recovery using a special metal structure. In some cases, suturing of the joint capsule and shortening or lengthening of the tendon is required.
If necessary, after diagnosing an x-ray, the angles of rotation can be adjusted. Recovery after such an operation can take several months.
Support function recovery
If the patient needs to restore support functions, osteotomy is performed on the hip joints. Here, a place is often created for the support of the hip bone.
The pelvic bones and the thigh itself are subjected to an incision. Such a surgical intervention is performed in the following cases:

Osteotomy for valgus and varus deformity of the lower leg
- the presence of congenital;
- when diagnosing false joints of the femoral neck;
- various deformations - or.
Several methods of bone dissection are also used here, depending on the goal of restoring the support function. The operation is performed exclusively under general anesthesia and requires several months of recovery.
The video clearly shows how a femoral osteotomy is performed:
Features of the operation and its consequences
An osteotomy is the cutting of a bone to improve a person's life.
But such improvements may not be noticed soon, especially since sometimes the operation, although it leads to the elimination of pain during the implementation of simple actions, but from the point of view of the cosmetic aspect, significant defects can be seen.
For example, the joints of the limbs will look asymmetrical, which can cause some discomfort to the operated person.
In addition, immediately after the operation, in most cases, long-term use of crutches (from one to three) months is required.
Despite the patient's uncomfortable position, the patient must take daily walks to restore the function of the operated bone.
The postoperative time is also accompanied by a course of physiotherapy, depending on the nature of the osteotomy. Full recovery can take up to a year.
Osteotomy can lead to certain complications, among which are revealed:
- The beginning of the process of suppuration of the wound- a special role in the presented situations is played by the immunity of the operated patient.
- Fragment Offset- occurs due to poor or incorrect fixation of them, which leads to a second operation.
- Delayed bone healing- based on the individual characteristics of the human body.
- Formed– impaired mobility of the operated bone and joint. A repeat operation is required.
 In connection with the foregoing, it is better to perform osteotomy only after strengthening the immune system, as well as with a professional surgeon who will not allow displacement or suppuration of the wound.
In connection with the foregoing, it is better to perform osteotomy only after strengthening the immune system, as well as with a professional surgeon who will not allow displacement or suppuration of the wound.
The osteotomy has one serious disadvantage. If it is necessary to repeat the operation associated with the replacement of the joint, it will be much more difficult to carry out such an action if the bone has already been dissected.
But in some cases, osteotomy is the only true, possible and reliable solution to eliminate the existing disease.
1The article is devoted to the topical issue of modern orthopedics - corrective osteotomies in the knee joint. The aim of the work is to review the current literature to summarize the data of domestic and foreign researchers, determine the indications for performing corrective osteotomies, the level and degree of correction of the axis of the lower limb. The results of studies of the influence of the position of the mechanical axis of the lower limb on the distribution of contact pressure in the joint are shown. Methods for determining the necessary degree of correction to achieve a normal mechanical axis of the lower limb are considered. Literature data on the results of normalization of axial deformities in the treatment of deforming arthrosis of the knee joint were analyzed. The use of this technique is advisable in young patients with gonarthrosis of the second or third stage. To obtain good long-term results, it is necessary to correctly and accurately follow the indications for performing corrective osteotomy, and to perform the most accurate calculation of the correction.
lower limb axis
gonarthrosis
corrective osteotomy
1. Bagirova, G.G. Osteoarthritis: epidemiology, clinic, diagnosis, treatment / G.G. Bagirova, O.Yu. Meiko. - M., 2005.- 224p.
2. Bragina, S. V. The structure of persistent disability in patients with gonarthrosis / S. V. Bragina, R. P. Matveev / / Orthopedic Genius. - 2011. - No. 4. - P.101-105.
3. Golovakha, M.L. Long-term results of high corrective osteotomy of the tibia in gonarthrosis / M.L. Golovakha, V. Orlyansky / / Orthopedics, traumatology and prosthetics. -2013. - No. 1. - P.10-15.
4. Zaitseva, E.M. Causes of pain in osteoarthritis and factors of disease progression (literature review) / E.M. Zaitseva, L.I. Alekseeva // Scientific and practical rheumatology. - 2011. - No. 1. - P. 50–57.
5. Zorya, V. I. Deforming arthrosis of the knee joint: a guide for doctors / V. I. Zorya, G. D. Lazishvili, D. E. Shpakovsky. - M.: Litterra, 2010. - 320 p.
6. Kolesnikov, M.A. Modern methods of treatment of gonarthrosis (literature review) / M.A. Kolesnikov, I.F. Akhtyamov // Bulletin of traumatology and orthopedics of the Urals. - 2012. - No. 1-2. - P. 121-129.
7. Kornilov, N.N. Modern ideas about the expediency of using corrective periarticular osteotomy in deforming arthrosis of the knee joint / N.N. Kornilov, K.A. Novoselov, T.A. Kulyaba // Bulletin of Traumatology and Orthopedics. N.N. Priorov. - 2004. -№3.-S. 91-95.
8. Kotelnikov, G.P. Surgical correction of deformities of the knee joint / G.P. Kotelnikov, A.P. Chernov. - Samara, 1999.- 180 p.
9. Loskutov, A.E. Arthroscopy and corrective osteotomy in the treatment of gonarthrosis / A.E. Loskutov, M.L. Golovakha // Visn. orthopedist, traumatologist that prosthesis. - 2002. - No. 2. − P. 5–7.
10. Makushin, V.D. Gonarthrosis: long-term results of the use of high valgus osteotomy of the tibia (review of foreign literature) / V.D. Makushin, O.K. Chegurov // Genius of Orthopedics. - 2007.- No. 1.- P.137-143.
11. Matveev, R.P. Osteoarthritis of the knee joint: problems and social significance / R. P. Matveev, S. V. Bragina / / Human Ecology. - 2012. - No. 9. - P. 53-62.
12. Mironov, S.P. Osteoarthritis: current state of the problem / S.P. Mironov, N.P. Omelyanenko, A.K. Orletsky // Bulletin of Traumatology and Orthopedics. N.N. Priorov. - 2001. - No. 2. - S. 96-99.
13. Muller, B. High tibial osteotomy: conditions, indications, technique, problems, results / V. Muller // MargoAnterior. - 2003. - No. 1−2. – S. 2−10.
14. Orlyansky, V. Corrective osteotomy in the area of the knee joint / V. Orlyansky, M.JI. Holovakha, R. Shabus - Dnepropetrovsk: Thresholds, 2009.- 159 p.
15. Planning the amount of correction for corrective osteotomy of the tibia / M.L. Golovakha, I.V. Shishka, O.V. Banit, V. Orlyansky// Orthopedics, traumatology and prosthetics.−2010.−№1.−S. 91–97.
16. A ten-to 15-year follow-up observation of high tibial osteotomy in medial compartment osteoarthrosis/ Yasuda K. //Clin.Orthop.Relat.−1992.−vol.282.−P.186-195.
17. Aglietti, P. Tibial osteotomy for the varus osteoarthritic knee/ P. Aglietti, E. Rinonapoli// Clin. Orthop.- 1983.-№176.-P. 239-251.
18. Agneskirchner, J.D.. The effects of valgus medial opening wedge high tibial osteotomy on articular cartilage pressure of the knee: a biomechanical study/ J.D. Agneskirchner // Arthroscopy.- 2007.-vol.23, No. 8.-R.852-861.
19. Amendola, A. High tibial osteotomy for the treatment of unicompartmental arthritis of the knee/ A. Amendola, L. Panarella // Orthop. Clin. North. Am. - 2005. - vol. 36, No. 4. - R. 497-504.
20. Arden, N. Osteoarthritis: epidemiology / N. Arden, M.C. Nevitt // Best Pract. Res. Clin. Rheumatol. - 2006.-vol.20, No. 1.-P. 3-25.
21. Association between valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee/ G.M. Brouwer, A.W. van Tol, A.P. Bergink, J.N. Belo, R.M. Bernsen, M.Reijman //Arthritis Rheum.- 2007.-vol.56, No. 4.-P.1204-1211.
22 Bae, D.K. Total knee arthroplasty following closed wedge high tibial osteotomy / D. K. Bae, S. J. Song, K. H. Yoon // International Orthopaedics (SICOT).- 2010. -vol.34.-P.283-287.
23. Brinkman, J.M. Osteotomies around the knee: patient selection, stability of fixation and bone healing in high tibial osteotomies/ J.M. Brinkman // J. Bone Jt. Surg. - 2008. - Vol. 90, No. 12. - R. 1548-1557.
24. Cole, B. Degenerative arthritis of the knee in active patients: evaluation and management / B. Cole, C. Harner // J. Am. Acad. Orthop. Surg. - 1999. - Vol. 7, No. 6. - P. 389-402.
25. Coventry, M. Proximal tibial osteotomy. A critical long-term study of eighty-seven cases / M. Coventry, D. Ilstrup, S. Wallrichs // J. Bone Jt. Surg. - 1993. - vol.75-A, No. 2. - P. 196-201.
26. Doherty, M. Risk factors for progression of knee osteoarthritis / M. Doherty // Lancet. - 2001. - Vol. 358. - P. 775.
27. Esenkaya, K. Proximal tibial osteotomies for the medial compartment arthrosis of the knee: a historical journey / K. Esenkaya, U. K. Akan // Strat. Traum. Limb Recon.−2012.−№7.−Р.13–21.
28. Frey, P. Closing-wedge high tibial osteotomy with a modified Weber technique/ P. Frey, M. Muller, U. Munzinger // Oper. Orthop. Traumatol.-2008.- vol.20, no.1.- P.75-88.
29. Frontal Plane Knee Alignment: A Call for Standardized Measurement / T. D. Cooke, E. A. Sled, R. A. Scudamore // J. Rheum.-2007.- vol. 34, No. 9. − P. 1796 - 1801.
30. Fujisawa, Y. The effect of high tibial osteotomy. An arthroscopic study of 26 knee joints / Y. Fujisawa, K. Masuhara, N. Matsumoto I IClin. Orthop. Surg. - 1976. - Vol. 11. - P. 576-590.
31. Giagounidis, E. M. High tibial osteotomy: factors influencing the duration of satisfactory function / E. M. Giagounidis, S. Sell // Arch. Orthop. Trauma Surg. - 1999. - vol.119, No. 7-8. - P. 445-449.
32. Hernigou, P. A 20-year follow-up study of internal gonarthrosis after tibial valgus osteotomy. Single versus repeated osteotomy / P. Hernigou // Rev. Chir. Orthop. - 1996. - Vol. 82, no. 3. - P. 241-250.
33. Hofmann, S. Principles and indications of osteotomies around the Knee/S. Hofmann, M. Pietsch// Arthroskopie.−2007.− vol.20, No. 4.−Р. 270-276.
34. Insall, J.N. High tibial osteotomy for varusgonarthrosis: a long term follow-up study/ J.N. Insall, D.M. Joseph, C. Lsika // J Bone Jt. Surg.- 1984.-vol.66-A, No. 7.-R.1040-1048.
35. Jackson, J. Tibial osteotomy for osteoarthritis of the knee /J. Jackson, W. Waugh // J Bone Joint Surg.-1961.- vol.43-B, no. 4.-P.746-751.
36. Jacob, R. Tibial osteotomy for varusgonarthrosis: indication, planning and operative technique / R. Jacob, S. Murphy // AAOS Instr. Course Lect. - 1992.-Vol. 41.-P. 87-93.
37. Karabatsos, B. Functional outcome of total knee arthroplasty after high tibial osteotomy/ B. Karabatsos, N.N. Mahomed, G.L. Maistrelli // Can. J. Surg. - 2002. - vol. 45, No. 2. - R. 116-119.
38. Koshino, T. Medial opening-wedge high tibial osteotomy with use of porous hydroxyapatite to treat medial compartment osteoarthritis of the knee/ T. Koshino, T. Murase, T. Saito// J. Bone Jt. Surg.- 2003.-vol.85-A, No.1.-R.78-85.
39. Kolb, W. Opening-wedge high tibial osteotomy with a locked low-profile plate / W. Kolb, H. Guhlmann, C. Windisch // J. Bone Jt. Surg.-2009.- Vol.91-A, No. 11.-R.2581-2588.
40. Lobenhoffer, P. Open valgus alignment osteotomy of the proximal tibia with fixation by medial plate fixator/ P. Lobenhoffer, J. Agneskirchner, W. Zoch //Orthopade.- 2004.- vol.33, No. 2.- P. 153-160
41. Maquet, P. Arthritis of the knee / P. Maquet. - New York: Springer-Verlag, 1980. - 183 p.
42. Moreland, J. R. Radiographic Analysis of the Axial Alignment of the Lower Extremity / J. R. Moreland, L. W. Basset, G. J. Hanker // J. Bone Jt. Surg.-1987.- vol. 69-A, No. 5.-P. 745-749.
43. Noyes, F.R. Opening wedge tibial osteotomy: the 3-triangle method to correct axial alignment and tibial slope/ F.R. Noyes, S.X. Goebel, J. West //Am. J. Sports Med. - 2005. - vol. 33, No. 3. - R. 378-387.
44. Paley, D. Principles of deformity correction/ D.Paley. − New York: Springer-Verlag, 2003. − 806 p.
45. Parvizi, J. Total knee arthroplasty following proximal tibial osteotomy: risk factors for failure / J. Parvizi, A.D. Hansen, M.J. Spangehl // J. Bone Jt. Surg.- 2004.-vol.86.- P.474-479.
46. Prospective outcomes of young and middle-aged adults with medial compartment osteoarthritis treated with a proximal tibial opening wedge osteotomy /R. F. LaPrade // Arthroscopy: The Journal of Arthroscopic and Related Surgery.−2012.−vol.28, №3.−P. 354-364.
47. Relationship between pain and medial knee joint loading in mild radiographic knee osteoarthritis/L.E. Thorp et al.//Arthritis Rheum.- 2007.- vol.57.- P. 1254-1260.
48. Rinonapoli, E. Tibial osteotomy for varusgonarthrosis: a 10- to 21-year follow-up study / E. Rinonapoli, G. Mancini, A. Corvaglia / Clin. Orthop. - 1998.-Vol. 353.-p. 185-193.
49. Sharma, L. The Role of Varus and Valgus Alignment in Knee Osteoarthritis/ L. Sharma // Arthritis Rheum.−2007.− vol. 56, No. 4.−Р.1044–1047.
50. Spahn, G. Complications in high tibial (medial opening wedge) osteotomy/ G. Spahn // Arch. Orthop. Trauma Surg.-2003.-vol.124.-P. 649–653.
51. Sprenger, T.R. Tibial Osteotomy for the Treatment of Varus Gonarthrosis: Survival and failure analysis to twenty-two years/ T. R. Sprenger, J. F. Doerzbacher /// J. Bone Jt. Surg.-2003.-vol.85-A, No.3.-P.469-474.
52. Ten-year results of tibial osteotomy for medial gonarthrosis. The influence of overcorrection / S. Odenbring // Arch. Orthop. Trauma Surg. – 1991.–vol. 110, no. 2. - P. 103-108.
53. W-Dahl, A. High tibial osteotomy in Sweden, 1998–2007. A population-based study of the use and rate of revision to knee arthroplasty/ A.W-Dahl, O. Robertsson, L. S. Lohmander// ActaOrthopaedica.− 2012.− vol. 83, No. 3.-P. 244–248.
54. Wildner, M. Complications of high tibial osteotomy and internal fixation with staples/ M. Wildner, A. Hellich, A. Reichelt // Arch. Orthop. Trauma Surg.–1999.–vol.111, No. 4. - P. 202-210.
55. Zaki, S.H. High tibial valgus osteotomy using the Tomofix plate –medium-term results in young patients/S.H.Zaki, P.J. Rae // ActaOrthop. Belg.-2009.- vol.75, no.3.-R.360-367.
Deforming diseases of the joints of degenerative-dystrophic origin are widespread among the adult population and account for more than 8-12%. In the structure of degenerative-dystrophic diseases of the joints, the knee joint accounts for 33.3% of cases. In recent years, there has been a tendency to increase the incidence of deforming arthrosis among people of young working age, which significantly increases the social significance of the problem. There is an increase in the incidence of arthrosis among people of the middle age group (40-60 years) up to 60%, and the duration of the period of disability increases. Conservative treatment does not always bring a positive effect, which leads to a decrease in the quality of life of patients. In young patients, the question of the need for surgical intervention is inevitably raised in order to prevent the progression of arthrosis and the transfer of knee arthroplasty to a later date.
Recently, operations to correct the axis of the lower limb for the treatment of gonarthrosis are again increasingly used, especially in young patients. It is known that corrective osteotomies have been used since the 19th century, when A. Meyer first used this technique for the treatment of gonarthrosis. In the 20th century, J.P.Jackson, W.Waugh, M.Coventry, T.Koshino, P.Maquet made a great contribution to the popularization of corrective osteotomies. Currently, R. Lobenhoffer is actively promoting the use of these operations.
Since the second half of the 20th century, in the treatment of gonarthrosis, knee arthroplasty has become the method of choice among surgical interventions. Corrective osteotomies, as a method of surgical intervention, have faded into the background, if not completely forgotten. In this article, we will try to consider the views of orthopedists on the use of osteotomies in the treatment of degenerative-dystrophic diseases of the knee joint.
Today, deforming arthrosis is recognized as a polyetiological disease. Many scientists studying the pathogenesis of osteoarthritis are supporters of the mechano-functional theory of the development of deforming arthrosis of the knee joint. According to this theory, the development of a degenerative-dystrophic process in the articular cartilage, subchondral bone, and joint capsule is associated with a functional overload of the cartilage due to a large amount of load. Axial deformities lead to premature disproportionate wear of the knee joint with the development of degenerative-dystrophic changes. Some scientists have expressed the opinion that the disease is based on a discrepancy between the functional load on the cartilage and its biological capabilities.
The influence of the position of the mechanical axis of the lower limb on the distribution of contact pressure in the joint has been the subject of a number of experimental studies. The most modern method for studying contact pressure is the use of a measuring foil, which operates on the basis of the Tekscan-System electromechanical resistance principles (Fig. 1.). Riegger-Krugh investigated the distribution of loads in the knee joint after osteotomies on cadaveric material. Modeled varus deformity, and then performed osteotomy. The authors found an expected increase in loads in the medial region with varus deformity and in the lateral region with valgus deformity. The work is interesting in that with the neutral axis of the knee joint, the load fell more on the lateral part of the joint. After correction, the same load data are obtained as with the normal axis.

Rice. 1. Examination of pressure distribution in the knee joint using the Tekscan-System.
The idea of corrective osteotomy is that due to the normalization of the axis of the lower limb, the load is redistributed from the damaged section of the joint subjected to significant loads to a relatively healthy one. Osteotomies in the area of the knee joint are divided according to the level of correction: at the level of the femur; at the level of the lower leg - high and low tibial, and are also divided according to the method of crossing the bone and the nature of the correction: transverse, spherical, straight, oblique, opening, closing. Currently, the most commonly used high opening wedge osteotomy, which allows you to solve almost all the technical difficulties that arise when normalizing the axis of the lower limb. It should also be noted the importance of using adequate, stable fixators when fixing bones after osteotomy. Previously, after the normalization of the limb axis by surgery, patients were forced to use various methods of immobilization for a long time, which significantly lengthened the rehabilitation period. In the 2000s, at the height of the new development of osteotomies, many manufacturing companies offered their fixation options, which can significantly reduce the recovery time after this operation. The use of modern fixators makes it possible to start a partial load on the limb in the first days after the operation and, of course, to exclude long-term immobilization, and in some cases to refuse it.
Corrective osteotomies are considered as a complementary method, preparing for arthroplasty, and in some cases, axis correction operations can do without prosthetics. In order for corrective osteotomies in the area of the knee joint to bring a lasting effect, it is necessary to: correctly determine the indications; adequate preoperative examination; calculate the degree and level of correction.
A good result in the correction of the axis of the lower limb can only be obtained with the right choice of indications. If corrective osteotomy is performed without taking into account the necessary factors, at best it can do no harm, and at worst, accelerate the destruction of the joint. The experience of modern orthopedists was summarized in 2009 at a meeting of the International Society of Arthroscopy, Knee Surgery and Orthopedic Sports Medicine and is reflected in Table 1.
Table 1
Indications, relative indications and absolute contraindications for corrective osteotomies
|
Indications |
Relative readings |
Absolute contraindications |
|
Age up to 60 years |
Age after 60 years |
Rheumatoid arthritis |
|
Deforming arthrosis 2 tbsp. |
Deforming arthrosis 3 tbsp. |
|
|
Absence of patellofemoral arthrosis |
Moderate patellofemoral arthrosis |
Patello-femoral arthrosis 3 tbsp. |
|
Varus, valgus< 15 гр. |
Instability of PKS, ZKS. |
Arthrosis of the contralateral joint. |
|
Isolated arthrosis 2-3 tbsp. |
Isolated arthrosis 3-4 tbsp. |
Osteoporosis |
|
Range of motion>100 gr. |
Range of motion >90 gr. |
Flexion limit >25 gr. |
|
Full extension |
Contralateral meniscectomy |
|
|
High degree of initial activity |
Meniscectomy |
Decreased blood flow through the vessels of the n / limb |
|
Normal contralateral joint component |
Dissecting osteochondritis |
Extra-articular deformities |
|
Stable knee joint, intact cruciate ligaments |
Necrosis of the condyles of the femur |
Decreased bone regeneration |
|
Intact menisci of the knee joint |
Flexion limit > 15 gr. |
Previous infection |
|
Varus, valgus deformity more than 15 gr. |
As a preparation for surgical treatment, it is necessary to conduct a thorough examination before the intervention, which includes clinical and laboratory tests, and, according to most orthopedists, it is imperative to perform images of the lower limb throughout - a teleroentgenogram (FLFS) (Fig. 2).
Rice. 2. Pictures of the lower limb throughout.
To correctly determine the level of osteotomy and the degree of necessary correction on images of the lower limb throughout, it is necessary to distinguish between the relationship of the following axial ratios and angles in the knee joint area (Fig. 2):
Anatomical-mechanical angle (AMU) = 6±1° - the angle between the anatomical and mechanical axes of the femur (1).
Mechanical distal femorolateral angle (MDFLU) = 87±3° (2).
Mechanical proximal mediotibial angle (MPMT) = 87±3°(3).
The anatomical axis of the lower limb (4) corresponds to the longitudinal axes of the femur and tibia.
The mechanical axis of the lower limb (Mikulich line) (5) passes through the center of the femoral head, through the center of the knee joint and through the center of the ankle joint.
Anatomical femorotibial angle (AFTU) = 173-175° - this angle is formed by the anatomical axes of the femur and tibia (6).
The line of the knee joint in the frontal plane has a bevel relative to the midline of about 2 degrees from the outside inwards (7).
Tibial slop 5-10° - posterior slope of the tibial plateau.
The main indications for performing corrective osteotomies in the area of the knee joint are: displacement of the mechanical axis of the lower limb medially or laterally by 10 mm from the midline, as well as a change in MDFLU and MMPTU by more than 3 degrees.
There are many methods for determining the degree of correction required to achieve a normal mechanical axis of the lower limb. One of the very first calculation methods was proposed by Coventry, which consists in calculations along the anatomical axis or along the biomechanical axis. Of the more modern techniques, it is necessary to note preoperative planning according to Lobenhoffer, in which it is necessary to focus on the passage of the mechanical axis through the Fujisawa point. The most commonly used preoperative planning is Miniation. Its essence is as follows: a radiograph of the entire lower limb is needed, planning also takes place taking into account the Fujisawa point. The Fujisawa point is an anatomical landmark located on the mechanical axis of the lower limb on the plane of the tibia through a point in the lateral compartment at a distance of 62% of the total width (provided that the countdown starts: from 0% of the medial edge to 100% at the lateral edge), which is the best location for the corrected mechanical axis (Fig. 3). This is consistent with the results reported by Noyes. The scientists obtained the same results, indicating that the shift of the load to the medial third of the lateral compartment reduces the degenerative change of the articular cartilage, while some restructuring of the cartilage layers is observed.

Fig.3. Anatomical landmark - point Fujisawa.
When planning by Miniazi, the following auxiliary lines must be used:
Line 1 runs from the femoral head (from its center) through the Fujisawa point of the total width of the tibial plateau lateral to the center of the knee joint to the plane of the ankle joint. This line represents the desired postoperative limb axis.
Line 2 starts from the center of the proposed osteotomy - point "D", which is the final planned osteotomy. This line goes down and connects the point "D" with the center of the ankle joint on the radiograph.
Line 3 connects point "D" with a point on line 1, which is located at its intersection with the plane of the ankle joint.
The open angle between lines 2 and 3 (Angle Alpha) is the desired angle for the required correction (Fig. 4).

Rice. 4. Planning the amount of correction according to Miniazi.
Only by using the correct indications and carefully calculating the degree of correction can positive and long-term results be expected. When analyzing literature sources, the following data on the effectiveness of osteotomies were obtained (Table 2).
table 2
Long-term results of corrective osteotomies
|
Quantity |
Result |
|
|
86% saving effect 5 years 74% saving effect 10 years 56% saving effect 15 years |
||
|
85%good 5 years 63% good 9 years old |
||
|
88% good 7 years old 78% good 10 years 57% good 15 years old |
||
|
Billings |
85% good 5 years 63% good 10 years |
|
|
87% good 5 years 69% good 10 years |
||
|
94% good 5 years 85% good 10 years 68% good 15 years old |
||
|
80% good 10 years 10% good 15 years |
||
|
80% good 5 years 58% good 10 years |
||
|
88% good 6 years old 63% good 10 years |
||
|
Matthews |
50% good, satisfactory 5 years 28% good 9 years |
|
|
51% good 9 years |
||
|
55% good 15 years |
||
|
81% good 11 years old |
||
|
91% good 5 years |
||
|
73% good 9 years old |
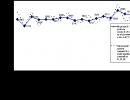
The data of the Swedish registry for 1998-2007 shows a generalized result of performing corrective osteotomies (3161 operations) and subsequent total knee arthroplasty (Fig. 5).

Fig.5. Endoprosthetics after corrective osteotomy (Swedish registry data).
The researchers note that during this period of observation, radiographically revealed no signs of progression of arthrosis, and only sometimes they note some deterioration in the contralateral section of the joint.
The results of studies on the use of total knee arthroplasty after corrective osteotomy were analyzed. There are publications on the difficulties of using arthroplasty after corrective osteotomy, in which an increase in the number of complications up to 30% is noted. Nevertheless, most orthopedists are inclined to believe that when performing correctly calculated osteotomies, primary arthroplasty does not differ in any technical features. Moreover, the implantation of the endoprosthesis in the conditions of normal anatomy of the knee joint brings the best long-term results.
And the last of the issues regarding osteotomies, which is widely covered in the literature, is complications. Complications of corrective osteotomies include progression of the process, lack of consolidation, infection, loss of correction, neuropathy of the tibial nerve.
Thus, in conclusion, we can say that corrective osteotomies, as a method of treating gonarthrosis, are still relevant. It is advisable to use this technique in young patients with gonarthrosis of the second or third stage. In addition, it is necessary to correctly and accurately observe the indications, calculate the correction, which allows you to get good long-term results.
Reviewers:
Yezhov I.Yu., Doctor of Medical Sciences, Head of the Trauma and Orthopedic Department, Associate Professor of the Department of Surgery, Nizhny State Medical Academy, FBUZ "Privolzhsky District Medical Center" of the Federal Medical and Biological Agency, Nizhny Novgorod.
Korolev S.B., Doctor of Medical Sciences, Professor, Head of the Department, State Budgetary Educational Institution of Higher Professional Education "NizhGMA" of the Ministry of Health of Russia, Nizhny Novgorod.
Bibliographic link
Zykin A.A., Tenilin N.A., Malyshev E.E., Gerasimov S.A. CORRECTIVE OSTEOTOMY IN THE TREATMENT OF GONATHROIS // Modern problems of science and education. - 2014. - No. 4.;URL: http://science-education.ru/ru/article/view?id=14032 (date of access: 01.02.2020). We bring to your attention the journals published by the publishing house "Academy of Natural History"