Scattered wikipedia sclerosis. Treatment of multiple brain sclerosis with drugs and folk remedies.
Multiple sclerosis (PC): Why appears, signs, diagnostics, course, therapy, cure or not?
All materials on the site are published under the authorship, or by the editors of professional doctors,
But are not a prescription for treatment. Contact specialists!
Sometimes we meet people suffering from this disease in the street or elsewhere, while they can still walk. One who for any reason came across multiple sclerosis (RS or, as neurologists write, SD - SClerosis Disseminata) recognizes it immediately.
Nociceptive pain
Strong pain in the root is strong pain, radiating roots or roots of the spinal nerve, which occurs without a nervous root present in pathology. Probably the cause of his formation is the outbreak of demyelinization in the spinal back of the spinal brain. The pain associated with the optical neuritude was rarely evaluated. The cause of pain in this symptom is inflammation, progressing in the nerve, where the activation of intracellular nociceptors is carried out by the nerve neurosis of the neurotransmitter. Such a pain mechanism can be characterized by a blunt character of pain.
In the literature you can find information that multiple sclerosis is a chronic process leading to disability, but it is hardly a patient to count on a long life. Of course, it depends on the form, not all of them are equally progressing, but the longest life of the sclerosis is still small, just 25-30 years with a remitrating form and constant treatment. Unfortunately, it is almost the maximum term that is far from all.
Symptoms of the neuritis of the optic nerve include one-way shoulder pain, which develops for several hours, is intensified when the eye moves, accompanied by one-sided problems of vision. There are some disputes on how to treat neuritis of the optic nerve. According to some authors, the oral use of corticosteroids is indicated, while others recommend using these drugs on the intravenous path.
The use of interferon often causes polymalgia, may also cause headaches; Chronic use of steroids can lead to osteoporosis and the emergence of complications in the form of pathological fractures. Muscle weakness or spasticity can cause posture defects.
Age, floor, form, forecast ...
Life expectancy - 40 or more years - the phenomenon is extremely rare, because in order to establish this fact, you need to find people who are sick in the 70s of the 20th century. And in order to determine the prospects for modern technologies, you need to wait 40 years. One thing is laboratory mice, another person. Hard. When, with a malignant RS, some die in 5-6 years, while the sluggish process allows a person to stay quite a long time in an active able-bodied state.
Typically, symptomatic treatment is recommended for other types of muscular-skeletal pain. Headaches are all headaches, regardless of whether they are caused by irritation of tires, vessels, muscles or other tissue receptors, characterized by nociceptive pain. Compared patients without headaches with a group of headaches.
There were reports about the severity of migraine during exacerbation. The occurrence of demyelinizing lesions in the upper segments of the spinal cord can cause acute forms of triple autonomous headache and occipital neuralgia. This may occur with one or both sides, usually with a passive cutting of muscles, which lasts less than 2 minutes. This symptom is not always painful, but almost half of the patients who have it, it is quite intense.
RS usually debuts at a young age, for example, at 15 years and to 40less often 50, although there are cases of disease in childhood and on average, for example, after 50. However, despite the fact that multiple sclerosis does not apply to rare diseases, the expansion of age boundaries does not happen and often, so the emergence of multiple sclerosis Children are considered to be an exception rather than the rule. In addition to age, RS prefers female sex, however, like all autoimmune processes.
The symptom occurs in the central nervous system as a result of increased activity of the central nervous systemcaused by damage to the inner bag, legs, an extended core. Changes can also occur in the spinal cord. It is believed that this symptom is due to the ephemeral propagation of spontaneous discharge generated by the axons, which were demoelinated. Therefore, it seems that the use of drugs that block sodium channels depend on voltage will be ideal treatment.
One of the randomized controlled studies has demonstrated the effectiveness of intravenous lidocaine and oral mexyleneboard in the treatment of these states. The cause of nociceptive pain in the presence of painful tonic contractions may be temporary ischemia, which arises as a result of muscle contraction. Some authors believe that these cancer may be useful for cannabinoids, which can affect both neuropathic and nociceptive components of this type of pain.
Patients die often from infections (Urosepsis, pneumonia), called intercurent. In other cases, the cause of death becomes bulbar disorders, under which swallowing, chewing, function of the respiratory or cardiovascular system, and pseudobulbar, and accompanied by violation of swallowing, facial expressions, speeches, intelligence, but cardiac activity and respiration does not suffer. Why this disease occurs - there are several theories, but its ethiology is not fully understood.
Spasty or increase in muscle tone or muscle rigidity are associated with a spinal cord injury. Some movements can increase spasticity or call spasms. Although the cause of pain tested by patients with spasms occurs in peripheral receptors, the central nervous system plays important role In achieving a good answer, because reduction of spasticity reduces pain associated with it. Oral ballopen was used for many years in the treatment of spasticity. In cases of refractory oral treatment, it is possible to consider the use of epidural anesthesia.
Forms and Patomorphological Changes of the Nervous System
The symptoms of multiple sclerosis are very dependent on which zone there is a pathological process. They are due to three forms located in different stages of the disease:
- Cerebrepinal, which is rightfully considered the most common, because the frequency of occurrence it comes to 85%. In this form, multiple already appear in the earliest stages of the disease, which lead to the affix of white substance and the dorsal, and brain;
- Cerebral, including cerebellar, eye, stem, cortical species flowing with the lesion of the white matter of the brain. With the progressive flow with the appearance of a pronounced jitter from cerebral form, one more: hyperkinetic;
- Spinal, for which the spinal lesions are characteristic, where, however, the more often suffers from the chest department;
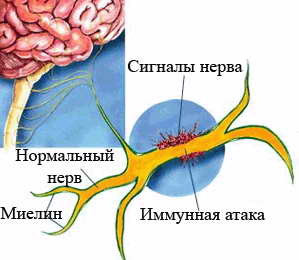
Patomorphological changes with multiple sclerosis are associated with the formation of multiple dense red-gray plaquesForming foci of demyelinization (myelin destruction) of pyramid, cerebelling paths and other CNS departments (central nervous system) or peripheral nervous system. Plaques are sometimes merged between themselves and reach quite impressive sizes (several centimeters in diameter).
Tizandine can also be effective when treating spasticity. There are also separate messages about the effectiveness of gabapentin or pregablin in the treatment of pain associated with spastic. Cannabinoids can also be useful at this type of pain. Literature on the use of other drugs, such as diazepams, clonazepams, Dantrolren or Botulinical toxin A, can be found in the literature.
The treatment of multiple sclerosis may also cause pain. The use of interferon beta can cause flu-like symptoms that occur from big group patients. Some of them describe these diseases as muscle pain that can be saved up to several months.
On the affected areas (the focus of multiple sclerosis) accumulates, mainly T-helpers (when the content of T-suppressors in peripheral blood), immunoglobulins, mainly IgG, while for the center of the center of the sclerosis, the presence of IA-antigen is characteristic. The exacerbation period is characterized by a decrease in the activity of the complement system, namely, its components C2, C3. To determine the level of these indicators, specific laboratory tests are used to help determine the diagnosis of PC.
This may affect 2-41% of patients who received interferon. Patients who received the Glakiramer acetate and Natalizumab did not increase the frequency of headaches. Chronic administration of glucocorticoids can lead to osteoporosis and the emergence of ailments related to its consequences.
Effective treatment of pain in patients with multiple sclerosis
Current recommendations for the treatment of central neuropathic pain also do not recommend these drugs. Secondary preparations include opioids and tramadol. In the treatment of neuralgia of a trigeminal nerve, the preparation of the first choice is carbamazepine. Beta therapy Interferon can cause influenza symptoms in most patients who received this medicine. In several studies, a decrease in these symptoms was shown after the administration of paracetamol interferon, ibuprofen and prednisolone.
Clinical manifestations, or rather, their absence, the duration and severity of remission of SClerosis Disseminata are determined by the coming intensive treatment and the corresponding reaction of the body - reeselinization.
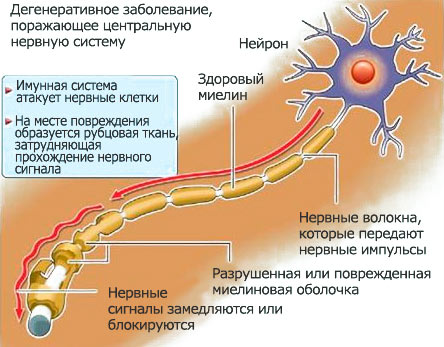
It should be noted that to other forms of sclerosis of the RS does not have a relationship, although it is called sclerosis. Many people explaining their forgetfulness inherent for old age refer to sclerosis, however, in the case of multiple sclerosis, although the intellectual abilities of a person suffer, but it has a completely different (autoimmune) mechanism and occurs at all other reasons. The nature of the plaques and PC are different and if the clerical damage of the vessels (!) Is due to the deposition of cholesterol (low density lipoproteins - LDL), then in this situation foci of demyelinization arise as a result of replacing normal nerve fibers on connective tissue. Foci is dissipated arbitrarily in various zones of the head and spinal cord. Of course, the function of this area is significantly violated. Detect plaques can a myreo or.
What can be the cause of multiple sclerosis?
Discussions, defending this or that point of view regarding the etiology of multiple sclerosis, continue to this day. the main roleHowever, belongs to autoimmune processeswho are considered the main cause of the development of PC. Violation in the immunity system, or rather, an inadequate response to some viral and bacterial infections is also not discharged by many authors. In addition, the prerequisites that promotes the development of this pathological condition include:
The most suitable therapeutic approach is an individual approach to each patient and the use of multi-directional treatment, which is focused on the pain mechanism, taking into account the expectations of a particular patient and therapist-therapist in its case. Often analgesic treatment is reduced to the use of individually selected pharmacotherapy. It is also worth remembering the possible additional treatment, including methods of rehabilitation and neuromodulation, which in some cases help maintain physical form and reduce pain.
- The impact of toxins on the human body;
- Increased level of radiation background;
- The effect of ultraviolet radiation (in white-skinned lovers of the annual "chocolate" tan, obtained in southern latitudes);
- Geographical location of the area of \u200b\u200bpermanent residence (cold climatic conditions);
- Permanent psycho-emotional tension;
- Operational interventions and injuries;
- Allergic reactions;
- Lack of visible cause;
- The genetic factor on which I would like to especially stop.
SD does not apply to hereditary pathology, so it is not at all necessary that a sick mother (or father) will be born a obviously sick child, however, it has been reliably proven that the NLA system (histocompatibility system) has a certain meaning in the development of the disease, in particular, the Lokus antigens A (HLA-A3), Locus B (HLA-B7), which, when studying the phenotype, the patient with multiple sclerosis is detected almost 2 times more often, and D-region - antigen DR2, determined in patients up to 70% of cases (against 30-33% in Healthy population).
Literature: Agostoni E. Frigerio R. Protti a.: Contradictions in the diagnosis of pain in the area of \u200b\u200bneuritis. Chronic pain in people with multiple sclerosis. Report Subcommittee on the quality standards of the American Academy of Neurology. Symptomatic trighemal vegetative headache associated with allodynia in patients with multiple sclerosis. Trigeminal neuralgia: pathology and pathogenesis.
K.: Headaches in patients with multiple sclerosis can mean an inflammatory process. Scattered sclerosis of central pain disorders. Psychosocial factors associated with the intensity of pain associated with the patient with interference and psychological functioning in people with multiple sclerosis and pain. The use of biotrophe in the treatment of spasticity with multiple sclerosis. This disease leads to a significant deterioration in the quality of life in all its spheres. Scattered sclerosis affects mostly young people.
Thus, it can be said that these antigens carry genetic information about the degree of resistance (sensitivity) of a certain organism to various etiological factors. Reducing the level of T-suppressors, overwhelming unnecessary immunological reactions, natural killers (NK cells) involved in cellular immunity, and interferon, providing normal operations immune systemThe sclerosis characteristic of multiple sclerosis may be due to the presence of certain histocompatibility antigens, since the NLA system genetically controls the products of these components.
The course of the disease in each patient may vary and depends on many factors, including the effectiveness of immunomodulatory treatment, which, unfortunately, is also limited. Advanced multiple sclerosis leads to a large number of complications, threatening life, such as aspiration pneumonia, chronic renal failure, urinary tract infections, urine disruption to maintain, depression or bedding.
For the first degree recognized symptoms of fatigue and fatigue, spasticity, vision problems, sphincter dysfunction, pain, cognitive disorders, sexual dysfunction, speech and swallowing problems. The symptoms of the second stage are: urinary tract infections, skin damage, damage to the system of articular, drowsiness, respiratory tract infection, violation of activities in everyday life. Symptoms of the third degree include: depression, mental disorders, social isolation, financial problems, family problems.
From the beginning of clinical manifestations to the progressive flow of multiple sclerosis

the main symptoms of the PC.
Symptoms of multiple sclerosis do not always correspond to the stage of the pathological process., exacerbations can be repeated with different intervals: at least a few years later, at least a few weeks. Yes, and relapse can last only a few hours, and it can reach a few weeks, but each new aggravation takes place heavier than the previous one, which is due to the accumulation of plaques and the formation of drain, exciting all new sites. This means that for SClerosis Disseminata is characterized by a remote course. Most likely, because of such inconstancy, neurologists came up with a different sclerosis name - chameleon.
The pain is one of the symptoms of the first degree, but also to the congratulations such symptoms of the second degree as skin damage, urinary tract infection or damage to bones and joints. Pain in patients with multiple sclerosis. It can be a peripheral or central neuropathic pain, receptor, idiopathic, yathedral or mixed pain. Progression of disease with limited mobility, fracture, dislocate, increasing spasms causes pain in the musculoser, especially when changing the position.
In this case, facilitate, in addition to properly selected physiotherapy, the adoption of an appropriate non-painful position for the patient. Pain syndromes like neuropathic pain in patients with multiple sclerosis. This is the most common neuralgia of the face. It occurs in 3-6 cases per 100,000 population. The pain is usually accompanied by local hyperalgesia of the skin. Appears in queues of violent attacks. Characteristic feature Neuralgia is the presence of trigger zones, that is, points or regions that even a minor touch causes painful attacks.
The initial stage is also not a certainty, the disease can develop gradually, but in rare cases can give a rather acute beginning. In addition, at an early stage, the first signs of the disease can not be noticed, since the course of this period is often asymptomatic, even if the plaques already take place. Such a phenomenon is due to the fact that with a few foci of demyelinization, healthy nervous fabric takes on the functions of affected areas and thus compensates for them.
The frequency of attacks ranges from several to a dozen or so a day, but over time they increase, and pain can change over time. The disease can continue from several weeks to several months and even years. Pain occurs on the one hand, although after the remission period may appear on the opposite side.
Triple triple neuralgia is extremely rare - in 2-5% of cases and never. If there is a neurological deficit between attacks, an organic disease should be considered. Periods of remission can last months or years. Over time, these periods become shorter and more painful, increasing intensity and duration.
In some cases Any one symptom may appear, for example, vision of vision for one or both eyes under cerebral form (eye variety) SD. Patients in a similar situation can not at all anywhere to treat or limit himself to a visit to an ophthalmologist, which is not always able to attribute these symptoms to the first signs of a serious neurological disease, which is multiple sclerosis, since the discs of optic nerves (zN) the color could not be changed With RS, the temporal half of the occasion pale). In addition, it is this form that gives long-term remissions, so patients may forget about the disease and consider themselves quite healthy.
The reason for the neuralgia of a trigeminal nerve remains unclear. In some patients, neuralgia can be caused by a nerve compression through the surrounding arch atherosclerotic brain artery, especially at the nerve penetration site into the bridge. Treatment of trigeminal nerve neuralgia.
The most effective anti-epileptic drugs, especially carbamazepine, and begin treatment should be launched. Using carbamazepine should control the function of the liver and control the level of sodium, which tends to decrease, especially in elderly patients. Carbamazepine is metabolized by 4 subtypes of cytochrome P450, therefore drugs that inhibit or induce cysts. Enzymes affect the efficiency and safety of its use. Carbamazepine reduces the half-life of Lusotezhina, and laxigin increases the effect of carbamazepine.
The basis of the neurological diagnosis - the clinical picture of the disease
The diagnosis of SClerosis Disseminata puts a neurologist, relying on the diverse neurological symptoms, manifested:
- Tremor of the hands, legs or the whole body, a change in the hand writing, it is difficult to keep some object in hands, and a spoonful of the mouth becomes problematic;
- Disruption of coordination of movements, which is very noticeable by gait, first the patients walk with a stick, and subsequently transplanted in a wheelchair. Although some still hard to do without it, as they themselves are not able to sit in it, so they are trying to move with the help of special devices for walking, based on both hands, and in other cases used with such a goal or stool with such a goal. What is interesting, for some time (sometimes quite a long time) they succeed;
- Nistagmom - the rapid movements of the eyes, which the patient, follow the movement of a neurological hammer in the left and right side, up and down alternately, cannot control itself;
- The weakening or disappearance of some reflexes, abdominal - in particular;
- A change in taste, a person does not respond to the favorite normal products and does not receive pleasure from food, so it will noticeably lose weight;
- Numbness, tingling (paresthesia) in hand and legs, weakness in the limbs, patients cease to feel a solid surface, lose shoes;
- Vegetative-vascular disorders (dizziness), why at first, dissipated sclerosis is differentiated and from;
- Dresses of the facial and triple nerve, which is manifested by the skeleton of the face, the mouth, the abnormal of the eyelids;
- Violation of the menstrual cycle in women and sexual weakness in men;
- Disorder of urination function, which is manifested by rapid urges in the initial stage and urine delay (by the way, and stool too) in the progression of the process;
- A transient decrease in visual acuity or both, bias in the eyes, losing sights, and in the future - retrobulbar neuritis (neuritis the visual nerve), which may end with full blindness;
- Chant (slow, divided into syllables and words) speech;
- Violation of motility;
- Disruption of the psyche (in many cases), accompanied by a decrease in intellectual abilities, critics and self-critics (depressive states or, on the contrary, euphoria). These disorders are most characteristic of the cortical species of the cerebral form of PC;
- Epileptic seizures.
Neurologists for diagnosing PC use a set of some signs. In such cases, symptoms characteristic of SD are used: Charcot Triad (jitter, nystagm, speech) and Pentada Marburg (jitter, nystagm, speech, disappearance of abdominal reflexes, pallor of optic nerve discs)
How to figure out the manifold of signs?
Of course, not all signs of multiple sclerosis may be present at the same time, although a cerebrospinal shape is distinguished by a special diversity, that is, it depends on the form, stage and degree of progression of the pathological process.
Usually, for the classical PC flow, the increase in the severity of clinical manifestations, which lasts 2-3 years to give the deployed symptoms in the form of:
- Paresis (functions of function) of the lower extremities;
- Registration of pathological stop reflexes (positive symptom of Babinsky, Rossolimo);
- Noticeable gait instability. Subsequently, patients are generally losing the ability to independently movement, but there are cases when patients cope with the bike, the main thing, holding the fence, sit on it, and then it went normally (it is difficult to explain such a phenomenon);
- An increase in the severity of trembling (the patient is not able to perform a pioneer sample - to get the tip of the nose with the index finger, and the knee-heel sample);
- Reduced and disappearance of abdominal reflexes.
Of course, the diagnosis of multiple sclerosis is primarily based on neurological symptoms, and laboratory studies are assisted in identifying diagnoses:
Confirms the diagnosis (MRI), as well as blood from Vienna and the Spinal Point, allowing to detect oligoclonal immunoglobulins (IgG), which are recognized by markers of sclerosis.
Disappointing diagnosis - SD
At the initial stages of the spinal shape of the sclerosis of it It should be differentiated from(The same paresthesias, the same weakness in the legs and even other times in pain). Other forms are also differentiated from many neurological and vascular diseases, so the diagnosis of PC takes time and continuous observation of the neurologist, which is possible only in stationary conditions. As a rule, the doctor is in no hurry to speak the patient about his suspicions, because he himself wants to hope for the best. Still, the doctor, although accustomed to everything, is also not easy to inform the person about such a serious illness, because the patient immediately goes shifting literature on this topic. And make their own conclusions.
The state of the patient man continues to deteriorate, however, who is rapid, who - not very (the disease can stretch for years), but it will be noticeable signs, because In the CNS there were irreversible processes.
The patient receives 2, and then 1 group of disability, as practically not capable of any work. With a remote (benign) form, a disability group can go in that order: 3, 2, 1 until the RS finally wins and will not take the top of the human body.
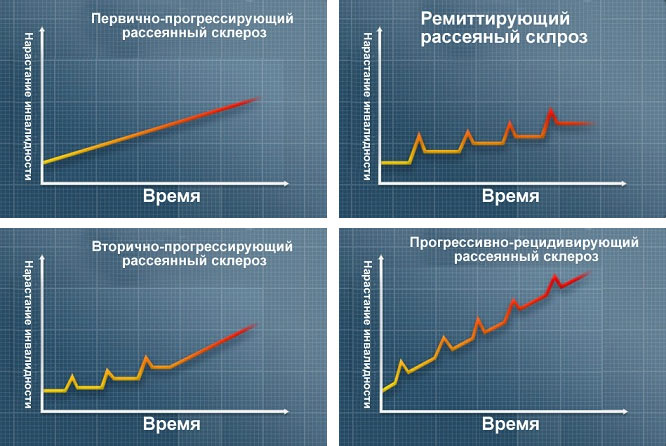
forms of the flow of PC
Meanwhile, each patient wonders: whether multiple sclerosis is heal? Of course, a person hopes that the medicine is already found, and he will hear a positive response, which, unfortunately, will still be negative. The pathological process with the help of modern treatment methods can be significantly suspended, but Medicine has not yet learned to cure completely PC. True, very High hopes scholars are associated with stem cell transplantationwhich, hitting the body, begin to restore the myelin shells of the nervous tissue to a normal state. It is clear that such treatment is not only very expensive, but also inaccessible, due to the special difficulty in the allocation and transplantation of them.
And yet it needs to be treated!
The treatment of multiple sclerosis also depends on the forms and stages of the disease, however there are general provisions that the attending physician adheres to:
- Purpose of therapeutic plasmapheresis. The procedure that entered into medical practice somewhere in the 80s of the last century has not lost its importance and in our time, since in most cases it is very beneficial for SD. Its essence is that the blood taken in the patient with the help of special equipment is divided into red blood (ermass) and plasma. The erythrocytic mass returns to the bloodstream of the patient, and the "bad" plasma containing harmful substances is removed. Instead, an albumin, donor freshly frozen plasma or plasma-substituting solutions (hemodez, reopolyglyukin, etc.) is injected with a patient;
- The use of synthetic interferons (β-interferon), which began to use at the end of the last century;
- Treatment with glucocorticoids: prednisone, dexamethasone, methipred, or ACTH - adrenocorticotropic hormone;
- The use of vitamins of group B, biostimulants and myelino-forming drugs: biosinax, kronssial;
- For additional treatment - the purpose of cytostatics: cyclophosphane, azatiotric;
- Adding muscle relaxants (Middokalm, Leiorzala, McCortex) to reduce high muscle tone.
It should be noted that in the 21st century, the treatment of multiple sclerosis is noticeably different from any years, say, 20 back. The breakthrough in the therapy of this disease was the use of new treatment methods that allow to extend remission to 40 or more.
In 2010, in Russia, the immunomodulatory drug of Cladribbin entered the medical practice (trade name - Movectro). One of the dosage forms - pills, very much like patients, besides, prescribe it courses 2 times a year (very convenient), but there is a "but": the drug is used exclusively in the case remisted flow Sclerosis scarked and is absolutely not shown in progressive form, so it is prescribed with extreme caution.
Recently, the popularity of drugs of monoclonal antibodies (MA) increases, which were synthesized in laboratory conditions and formed the basis of targeted treatment, that is, monoclonal antibodies (immunoglobulins - Ig) have the ability to affect only those antigens (Ag) that need to be removed from the body . Attacking myelin and binding to a certain specificity antigen, antibodies form complexes with this AG, which are subsequently removed, and, it became possible to harm it. In addition, Ma, hitting the patient's body, contribute to the activation of the immune system in relation to other alien, and therefore not very useful, antigens.
And, of course, the most advanced, most efficient, but the most expensive and far from all available is the latest technology used in Russia since 2003. This is a transplanting of stem cells (SC). Regenerating white substance cells, eliminating scars formed as a result of myelin destruction, stem cells restore the conductivity and functions of affected areas. In addition, the SC positively affect the regulatory ability of the immunity system, so I want to believe that the future - for them and multiple sclerosis will still be defeated.
Ethnoscience. Is it possible?
With multiple sclerosis It is hardly necessary to rely on the healing properties of plantsIf scientists all over the world are fighting for this problem. Of course, the patient can add to the main treatment:
- Honey (200 grams) with Luke Juice (200 grams), which will take 1 hour before meals three times a day.
- Or mummy (5 grams) dissolved in 100 ml of boiled (chilled) water, which is also taken on an empty stomach along a teaspoon 3 times a day.
 Even scattered sclerosis at home is treated with clover, which insists on vodka, decoction made of a mixture of hawthorn leaves, roots of valerian and root grass, drink a glass of boiled nettle leaves with a yarrow or use other vegetable components overnight.
Even scattered sclerosis at home is treated with clover, which insists on vodka, decoction made of a mixture of hawthorn leaves, roots of valerian and root grass, drink a glass of boiled nettle leaves with a yarrow or use other vegetable components overnight.
Everyone chooses at WISH, but in any case, self-treatment would well agree with the attending physician. But medical physical education With multiple sclerosis, you should not ignore. However, here should not be reed only on itself, excessive independence is absolutely nothing to do with this severe illness. The attending physician will select the load, the LFC instructor will teach the exercises corresponding to the state and capabilities of the body.
By the way, at the same time, the diet can be discussed. The doctor who treats is heavily gives his recommendations, but patients are often trying to expand their knowledge in the field of dietology, so they turn to the relevant literature. Diets such really exist, one of them developed a scientist from Canada Ashton Embami, where it represents a list of prohibited and recommended products (easy to find on the Internet).
Probably, we are not particularly surprised by the reader, if we note that The menu should be full and balanced, contain the required amount of not only proteins, fats and carbohydrates, but also to be rich in vitamins and trace elements, so vegetables, fruits and cereals must be included in the patient's diet. In addition, regular problems with intestines should be taken into account, accompanying multiple sclerosis, so it is necessary to try to ensure its uninterrupted work.
Step 1: Pay advice with the form →
You can increase the amount if your question is complex, requires a deep consideration and / or voluminous response (for example. Detailed analysis of tests, etc.).
Step 2: After payment, ask your question in the form below ↓At the end of the question do not forget to specify the payment code!
(otherwise you will not be able to identify)
Paid questions are usually processed within 48 hours
Multiple sclerosis(SIN: Multiple Sclerosis, Sclerosisdisseminata) - a chronic demyelinating disease that develops due to the effects of an external pathological factor (most likely infectious) on a genetically predisposed organism. In this disease, there is a multi-grade damage of the white substance of the central nervous system, in rare cases with the involvement and peripheral nervous system. In most cases, multiple sclerosis (PC) is characterized by steady, often a wave-like flow, which may be subsequently replaced by gradual progression.
Historically higher rates of prevalence (soreness) and the incidence of PC are found in geographical zones as much as possible from the equator. AT last years This dependence is expressed to a lesser extent, and multiple sclerosis began to meet in many southern regions. The direct connection between the spread of multiple sclerosis with breadth is most likely due not only geographical position, but also big amount Ethnic socio-economic features.
Depending on the prevalence of multiple sclerosis, three zones are isolated: a high risk area with a frequency of a disease of more than 50 per 100,000 population includes Northern and Central Europe, South of Canada and the North of the SSA, South of Australia and New Zealand. The medium risk area has a frequency of 10-50 per 100,000 population and combines the center and south of the SSA, the Hawaiian Islands, Northern Scandinavia, South Europe, Israel, White Population South Africa, North and West of Ukraine, the European part of Russia, the Far East. Low risk area with a frequency of 10 and less per 100,000 population includes Asia, North South America, Alaska, Greenland, Islands Caribbean, Mexico, most of Africa, Middle and Middle East. The main trend in the epidemiology of multiple sclerosis of the last decades is a distinct increase in prevalence and morbidity indicators in most regions.
In Russia, in addition to the historically established high-risk zones of multi-risk sclerosis in the north and north-west of the country, the high risk zones in the south of the European part, in the Volga region and the Far East, are described in the 1980s.
Feature geographical distribution sclerosis is the presence of small territories with very high levels Incidences (clusters) and single cases of a sharp increase in incidence rates (microepidemi events of the PC), among which the RS epidemic in the Faroe Islands (Denmark) is most well known after World War II.
In addition to geographical, a significant impact on the risk of developing sclerosis, features of nutrition, socio-economic and environmental characteristics are provided. Attention is drawn to age and sexual differences. RS is rarely diagnosed in patients under 15 and over 55 years old, although in recent years there has been an increase in cases of early debut of the disease under 15 years of age (10-12 years), which is 2-8% of total Patients with RS in different regions.
What provokes multiple sclerosis
Currently, multiple sclerosis is defined as a multifactorial disease. This means participation of both external and hereditary factors.
External factors , affecting genetically predisposed persons, can stimulate the development of a inflammatory autoimmune process in the central nervous system and the destruction of myelin. Infectious agents are likely to have the greatest importance, especially viral infections. Numerous studies have shown that, most likely, there is no one virus as root causes of multiple sclerosis. In this case, an increased titer of antibodies in serum and cerebrospinal fluid to various viruses was revealed, which may be a consequence of impairment impairment (polyclonal activation of humoral immunity), and not indicate the etiological significance of a particular pathogen.
Cory, rubella viruses, infectious mononucleosis (Epstein-Barra virus), herpes virus, and various bacteria can act as a trigger factor, participating in induction and maintain inflammatory and autoimmune processes. Much attention is paid to the participation of latent, persistent viral infection, including conditionally pathogenic viruses, in stimulating the immune system and reactivation of the pathological process. As triggers of exacerbations of multiple sclerosis, various ex- and endogenous factorsaffecting the permeability of the hematorecephalic barrier (GEB) separating the antigen brain of the barrier organ from the immune system of blood. Among these factors special meaning They may have injuries of head and back, stress, physical and mental overvoltage, operations. It is assumed that big influence The immunological and biochemical processes in the central nervous system have nutritional features, in particular the predominance of animal fats and proteins can be one of the additional risk factors for the development of multiple sclerosis. The additional pathological effect of exotomins, in particular paints, organic solvents, oil refining products, is not excluded.
Convincingly proven availability genetic factors the predisposition to multiple sclerosis, which is most clearly manifested in family cases of the disease. In families of patients, the risk of a second case of a disease in different ethnic groups is 4-20 times higher than in this population as a whole. Monosigitious twins RS meets 4 times more often than that of dialigid. Epidemiological and genetic studies revealed a connection between the risk of RS's development and certain loci of the main histocompatibility system on the 6th chromosome (HLA), which cause the originality of an immune response from this individual. Initial research by indirect methods revealed a connection with Lokusamp A3 and B7 from the first class. A stronger association is marked with a set of alleles by the second-class NLA Lo Kusus, which is inherited. This nabe called the name "Haplotype DR2 (or DW2). Studies using direct genotyping methods allowed to clarify its alllel composition, which is currently described as DRB1 * 1501, DQA1 * 0102, DQB1 * 0602. In addition to this haplotype, the only confirmed Association is the connection of the RS with DR4 in the residents of O.Sardinia (Italy). In addition to associations with NLA-system genes, possible connection between RS development risk with cytokine genes, Melin proteins, nonspecific enzymes, T-cell receptors, immunoglobulins, etc. Most likely, PC is a multigenic disease, for the development of which a combination of certain alleles is necessary for several genes. . Under influence external factors This hereditary predispoe exercise is implemented as a chronic demyelinizing process, activity and originality of clinical manifestations of which also depend on the individual set of external and genetic factors.
Pathogenesis (what happens?) During the dispel sclerosis
Of great importance in the pathogenesis of multiple sclerosis has the state of the immune system. This is evidenced by histological studies: the presence of infiltrates consisting of immunocompetent cells in a fresh plaque; communication with genetic factors controlling the immune system; a variety of changes in the indicators of immunological reactions of blood and cerebrospinal fluid; The ability of immunosuppressants to suppress the aggravation of the disease and, finally, the presence of antibodies and clones of cells specific to brain antigens, among which the most encephalitogenic is the main protein of myelin (OBM). A small group of activated cells causes an increase in the permeability of the hematorecephalic barrier, which leads to the penetration of a large number of blood cells and the development of an inflammatory response to the brain fabric. Subsequently, the tolerance of myelin antigens and in the pathological process include various cellular and, to a lesser extent, humoral autoimmune reactions. Autoimmune reactions to the OMB and other antigens grow avalanche-like. The leading importance in starting and maintaining the immunopathological process has antigen-representing cells - microglia, astrocytes and endothelium of brain vessels that can attract circulating lymphocytes into fabric and activate them. Many glia cells, like blood cells, are able to produce activation cytokines, stimulating inflammatory and autoimmune reactions. Among the activation cytokines, gamma-interferon, the necrosis factor of alpha tumors, interleukins 1, 2 and 6 (IL1, IL2, IL6), which can enhance the expression of adhesion molecules and stimulate the representation of the antigen lymphocytes. The increase in cytokine products can occur under the influence of various external and internal factors, which reactives the pathological process. The dispute destruction of myelin can occur in various ways - activated cells, cytokines, antibodies. It is possible to switch immune reactions with external antigens on brain antigens (molecular mimicry mechanisms), the development of the reaction to the superantigs and polyclonal stimulation of immunity in case of insufficiency of control mechanisms for autoimmune reactions.
The possibility of direct cytopathic influence of viruses, cytokines is not excluded. The products of the decay of myelin and other toxic substances on oligodendrocytes (myelinsiticizing cells). Of great importance in the pathogenesis of multiple sclerosis have features of exchange in brain tissue, changes in the rheological properties of blood, as in any inflammation, disorders of the exchange of zinc, copper, iron and other micro elements, the exchange of polyunsaturated fatty acids, amino acids and other factors. At the same time, nervous fibers suffer, which are subjected to irreversible degenerative changes. Cytokines, peroxidation products and other substances can damage the nerve fibers in the early stages of the disease.
A long autoimmune process leads to the depletion of the immune system with the development of secondary immunodeficiency and a decrease in the hormonal activity of the adrenal cortex.
Patomorphology. The morphologically pathological process with PC is characterized by numerous focal changes in the head and spinal cord. Favorite localization of foci (or plaques) is a perivativericular white substance, side and rear cervical and chest ropes of spinal cord, cerebellum and brain stem. In these sections, the CNS is formed a large number of Frams of different sizes and shapes that differ from normal nervous tissue with color and consistency. Characteristic of the fresh plaque is perivascular infiltration of the brain tissue lymphoid elements of the blood, most of which are T cells, as well as the pronounced local edema, leading to early stages to the transient block of the nerve pulse along the affected fiber. The destruction of myelin and the subsequent degeneration of the axon are the causes of the stable nerve pulse block. The old, inactive plaque of multiple sclerosis, grayish color and tight to the touch, characterizes the following reactive of astro cytis (astroglyosis) and decrease in the content of oligodendrocytes. In some cases, on the edges of the old plaque, new edema zones and perivascular infiltration may be observed, which indicates the possibility of the growth of old foci.
Symptoms of sclerosis
In typical cases, the first clinical symptoms of multiple sclerosis appear in people of young age (from 18 to 45 years), although in lately Increasingly describe RS debut both in children and people over 50 years old. The first symptoms of the disease are often retrobulbar neuritis, a decrease in visual acuity, cattle, sensation of fuzziness of the image, shining in front of the eyes, transient blindness to one or two eyes (last with a bilateral process). The disease can begin with eye disorders (diplopia, squint, inter-identical ophthalmoplegia, vertical nystagm), neuritis of facial nerve, dizziness, pyramidal symptoms (central mono-, hemi or parapaperse with high tendon and periosal reflexes, stop clones, pathological pyramidic reflexes, disappearance Abdominal skin reflexes), cerebellar disorders (step-down when walking, static and dynamic ataxia, intentional jitting, horizontal nystagm), surface disorders (numbness, dis- and paresthesia) or deep sensitivity (sensitive attaxia, sensitive paresis, hypotension).
The earliest symptoms of the lesion of conductive paths can be fast depletion and disappearance of abdominal reflexes, a decrease in vibration sensitivity and dissecessia, asymmetry of tendon reflexes. Significantly less often in the first signs of the disease may be neurotic disorders, syndrome chronic fatigue, violations of the functions of pelvic organs (urination delay, imperative urge), as well as vegetative violations.
Analytical retrospective studies have shown that the debut of multiple sclerosis with retrobulbar neuritis and sensitive disorders and long-term first remission are signs of a more favorable course of the disease, while the appearance of signs of damage to the pyramidal path or cerebellum paths and the short first remission (or primary progressive flow, i.e. The absence of remission as a whole) are prognostically unfavorable. As a reflection of vegetative and endocrine disorders in women, there is a violation of the menstrual cycle, men have impotence.
The progression of multiple sclerosis leads to the defeat of other CNS departments and the emergence of new symptoms. Already in the initial stages are characterized by increased fatigue (syndrome of "chronic fatigue"). In later stages, psychopathological changes may manifest itself in the form of emotional instability, euphoria or depression, irritability, lethargy, apathy, reducing the intellect of varying dement to the dementia. Epileptic seizures at PC are rare, although some patients may have paroxysmal changes of tone, neuralgic pains and other paroxysmal sensitivity disorders. The most striking manifestation of sensory paroxysms under PC is "striking" by the type of Lermitta syndrome. Lermitta syndrome is expressed in the painful unpleasant feelings of tingling, voltage, "current passage" on the back from the head to the legs, more often when the neck is extension. The estimated reason is the focus of demyelinization in the spinal cord at the cervical level with severe edema. In this case, the mechanical deformation, for example, in the extension of the neck or activation of damaged pyramid fibers leads to irritation of sensitive fibers passing through this department, and the occurrence of peculiar sensations.
There are a number of symptom complexes characteristic of multiple sclerosis, reflecting the features of the clinical manifestation of the demyelinizing lesion. Among them are the most common syndromes of "clinical cleavage", "inconstancy of clinical symptoms" and "hot bath".
Syndrome "Clinical splitting", or "dissociation", was described by D.A. Markov and A.L. Leonovich. The authors understood this syndrome as a variety of manifestations of the inconsistency between the symptoms of the defeat of various conducting paths at the PC. This syndrome reflects a combination of one sick symptoms of damage to different conducting paths or different levels of lesion. For example, high tendon reflexes, pathological stop signs along with pronounced hypotonia in patients with PCs are observed with simultaneous damage to the pyramidal path and cerebellum conductors, less often - with a violation of deep sensitivity. One of the most famous and well-studied syndromes at PC is the hot tub syndrome. It is known that when the temperature is raised ambient The state of patients with RS is worsening. This syndrome is nonspecific and reflects the increased susceptibility of the nervous fiber, deprived of myelin shell ("insulation"), to external influences. All these changes, as a rule, are transient, unstable character, which is more specific to multiple sclerosis symptom than the deterioration of the state. For multiple sclerosis, the clinical phenomenon of the severity of the symptoms of the PC is not only for several months or years, but also for one day, which is associated with the large sensitivity of the demyelinized fiber to changes in homeostasis.
In general, clinical manifestationssclerosis scarmcan be divided into 7 main groups:
- the lesion of the pyramid system with hemi, para- and tetrapabs with a corresponding increase in tendon reflexes and pathological pyramidal symptoms;
- defeat cerebellum and its ways with the development of static and dynamic ataxia, muscle hypotension;
- sensitivity disorders, initially deep, with the development of sensitive attaxia and sensitive paresis, and then pain and temperature via conduction type;
- the lesion of the white substance of the brain stem with various violations of cranial innervation, most often with the development of glasses of glasses, the lesion of the facial nerve (peripheral paresis of the muscles of the face);
- newit of the optic nerve (including retrobulbar neurites) with a decrease in visual acuity and the appearance of cattle;
- violations of the function of the pelvic organs, more often by the type of imperative urges, urination delays, subsequently before urinary incontinence;
- neuropsychological changes, weakening of memory, euphoria or depression is characterized by chronic fatigue syndrome.
In most cases, patients have symptoms of damage and head, and spinal cord ( cerebrospinal shape ). In some cases, the symptoms of spinal cord lesions prevail in the clinical picture ( spinal shape ) or cerebellum ( cerebellum or hyperkinetic form ). In the latter case, the intentional jitter can be so pronounced that it reaches the degree of hyperkinase and makes it impossible any targeted movement. Distribution arise, adiadochokinesis, chant speech, expressed ataxia.
Flow. In 85-90% of patients, the disease has a wave-like flow with periods of exacerbations and remission, which, after 7-10 years of illness, almost all patients are replaced by secondary progression when there is a gradual deterioration in the state of patients. In 10-5% of cases of PC, from the very beginning, it has a primary progressive (progressive) current. The severity of the damage to the nervous system and the pace of development of irreversible symptoms varies significantly from different patients. Possible both cases of the "soft", "favorable" course of the disease with periods of remission or stabilization for dozens of years and the rapid electrical options ( trunk form sclerosis scarm , or Disease of Marburg ). The true exacerbation of PC should be differentiated from pseudo-plants, when the deterioration in a state of the patient is not associated with the activation of the immunopathological process, but with nonspecific changes in homeostasis. They are characterized by the temporary deepening of the symptoms already in the patient, and not the appearance of new ones. Subclinical exacerbations are possible, when new foci is formed in clinically dumb x zh (perivativericular e-substance) and are detected only with magnetic resonance imaging.
Different changes in homeostasis may be triggers provoking the aggravation of the disease. Often in this role are infections, psychogenic stresses, less often - injuries, supercooling and physical overvoltage, operations (especially under anesthesia), the effects of toxins and radiation. Perennial dynamic observations of sick women with PC in different countries of Europe showed that pregnancy and childbirth do not affect a short-term and long-term forecast for RS, and many patients induce the development of a rack long remission. Artificial interruption of pregnancy, especially at the later dates, is quite often the cause of heavy exacerbations of the PC.
Diagnosis of sclerosis sclerosis
Clinical polymorphism of PC, due to the individual set of external and genetic pathogenesis factors, causes significant difficulties early diagnosis. Since 1983, Diagnostic Criteria S. Poser is used to form a diagnosis of PC. According to these criteria, the disease should manifest itself under the age of 59 at least two foci of the lesion of the white substance CNS, the occurrence of which should be divided in at least one month.
The criterion of separation in localization and the formation of foci ("dissemination in place and time") is the main one when establishing clinically reliable diagnosisRS. It is important that all other reasons for such a multi-grade damage to the CNS should be excluded before establishing the diagnosis of the PC. In many cases, it is clinically unable to completely identify these criteria: there are symptoms associated with only one source, and the remittant course of the disease or clinical signs of the defeat of two simultaneously emerged foci in the white substance, etc. For accounting such cases, the concept has been introduced probablePC when the diagnosis can be confirmed or refuted after an additional examination.
In the diagnosis of PC, when there are clinical manifestations of only one focus with the characteristic wave-like process, the verification of the presence of several foci is important. Subclinical lesions of the conductors can be revealed by additional methods. The first group of methods is the neurophysiological methods of the caused potentials, allowing when changing latency and amplitude of the peaks of curves to diagnose damage to the corresponding conductor system (visual, somatosensory and short-prophent stem, caused by potentials). Neurophysiological methods allow you to identify subclinical foci and confirm the diagnosis of 50-60% of cases.
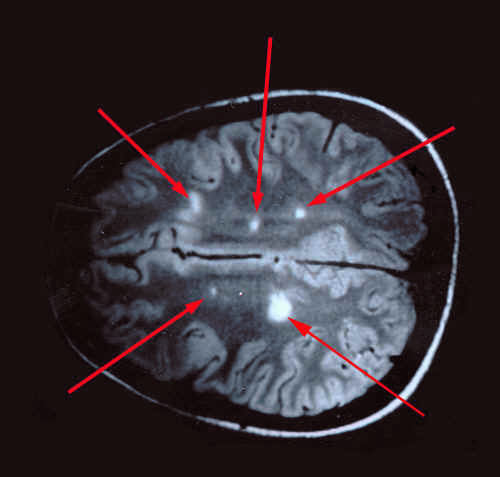
In 90% of cases, a multicag damage is confirmed with a magnetic resonance imaging of the brain, when a focal increase in signal intensity is recorded on T2-suspended images. Sometimes, with severe long-term processes, foci can be merged into the hyperfensivity zones, secondary atrophy of the brain substance is revealed.
High informative MRI study using a magnevoist and other contrast agents, as a rule, based on the Gadolinium (GD-DTR). Paramagnetic contrast enhances the signal from the zone of inflammation and edema (on T.-suspended images). This method allows you to identify fresh foci with an increase in the permeability of the BEB, i.e. Makes it possible to monitor the activity of the pathological process. Comparisons with data of pathomorphological studies made it possible to conclude that the increase in the contrast occurs solely in the fresh foci of demyelinization with severe inflammatory changes in the form of edema and cell infiltration.
The detection of a multi-decrepage lesion of the white matter of the brain on MRI is not the basis for the diagnosis of the PC: such changes may be observed at various neurological diseases. This method can be used as an additional, i.e. To confirm the clinical assumption of the diagnosis. A certain diagnostic value has the detection of increased IGGV cerebrospinal fluid products. With isoelectric focusing, these igration oligoclonal groups, so they got the name "oligoclonal immunoglobulins". This phenomenon is a consequence of the stimulation of humoral immunity, as well as an increased titer of antibodies to various viruses, i.e. Indicates certain impairment of immunoregulation in the brain.
Oligoclonal immunoglobulins in cerebrospinal fluid are characteristic of PC and are detected in 80-90% of PC patients. Therefore, a special section was introduced in the Pozer scale: "Laboratory confirmed" reliable or probable PC. At the same time, oligoclonal immunoglobulins can be detected in other inflammatory and certain infectious diseases of the nervous system (for example, with neurospection), indicating the presence of an immunopathological process in the central nervous system.
Indirect value have various changes in the indicators of immune responses of peripheral blood, indicating the presence of an imbalance in the immune system: a decrease in the content of T cells, especially the suppressor phenotype, a decrease in the functional activity of specific and nonspecific suppressors, the relative increase in cell content and the signs of their polyclonal activation Invivoble levels of products of activation cytokines and antibodies to Obm. These changes make it possible to more determine the activity of the pathological process, but do not have independent diagnostic value, as they vary significantly from each patient. In blood, leukopenia, neutropenia, and in the exacerbation stage - lymphocytosis are often detected. There is an increase in platelet aggregation, the trend towards an increase in fibrinogen content and at the same time activation of fibrinolysis. With the exacerbation and progressury of the course of the disease, a violation of the function of the cortex of Chechnyko is revealed, manifested by a sharp decrease in excretion with urine C21 corticosteroids (especially glucocorticoid fraction), a decrease in the level of cortisol in the blood plasma. During remission, the content of steroid hormones in the urine and cortisol in plasma is often refunded to the norm.
The Differentiation of the PC in the initial stages follows from neurotic disorders, vegetative-vascular dysfunction, labyrinthitis, or minor syndrome, the optical neuritis of various etiologies, tumors of the head and spinal cord, acute scattered encephalomyelitis, encephalitis of various etiology, degenerative diseases of the central nervous system.
PC spinal shapes must be differentiated from spinal cord tumors. In contrast to the tumor, the spinal symptoms of the PC in the initial stages is characterized by a smaller severity of the paresis (spask dominates against the background of severe pathological pyramidal symptoms), sensitivity disorders and the functions of the pelvic organs. In diagnostic complex cases The necessary information is given by the lumbar puncture (the presence of a block of the subarachnoid space and a sharp increase in protein content during spinal cord tumors), contrasting research methods and MP tomography. A differential diagnosis of PC and progressive degenerative diseases of the nervous system may be difficult. Thus, the hyperkinetic form of multiple sclerosis can resemble the shape of hepatocerebral dystrophy, cerebelchok ataxia. In pronounced lower paraparene, the presence of a pitch disease should be eliminated, at which there are no signs of the defeat of other parts of the nervous system. The final judgment in favor of this or that disease in many cases can only be done based on dynamic observation of patients.
Treatment of dispel sclerosis
Due to the fact that the etiology of the disease is unclear, the etiotropic treatment of the PC is currently not. The principles of treatment of patients with PC are based on an individual approach, taking into account the degree of activity of the immunopathological process at each specific moment in this patient, the duration of the disease, the degree of severity of individual neurological symptoms. Pathogenetic treatment is aimed at combating the exacerbation or progression of the disease and includes mainly anti-inflammatory and immunosuppressive drugs, pathogenetic therapy aims to prevent the destruction of the brain tissue with activated cells of the immune system and toxic substances. The appointment of immunomodulating drugs with PC patients should be carried out strictly individually based on and under the control of immune status and taking into account all the testimony and contraindications, including the definition of the activity of the immunopathological process at the time of the intended immunocorrection. In recent years, a group of new drugs appeared, capable of long-term use to reduce the frequency of exacerbations and slow down the progression of the disease, i.e. Providing preventive action. Of great importance are adequately selected symptomatic treatment, the medical and social rehabilitation of patients. Symptomatic therapy is aimed at maintaining and correction of the functions of a damaged system, compensation of existing disorders. Of great importance is a group of metabolic preparations that contribute to the regeneration of damaged myelin and strengthening their own mechanisms for monitoring the immunopathological process.
Pathogenetic therapy. With the exacerbation of the disease, corticosteroids and drugs of adrenocorticotropic hormone (ACTH), which have anti-inflammatory and immunosuppressive effect remain with the preparations of choice. The purpose of these drugs is intended to limit inflammatory and autoimmune processes and the degree of destruction of myelin, i.e. Improve the condition of patients at the time of exacerbation, reduce the duration of exacerbation and prevent the development of persistent neurological consequences. Corticosteroids practically do not affect the pathological process in the subsequent. Most clinical trials proved their effectiveness mainly with exacerbation of a remote course of the disease. It should be emphasized that the long-lasting intake of corticosteroids perosimes a large number side Effects, among which it is possible to distinguish the suppression of blood formation, osteoporosis, the formation of an ulcers.
The greatest distribution currently received short courses of large doses of soluble corticosteroids, which can be administered intravenously during the acute stage of activation of the pathological process. With this scheme of administration, there is significantly fewer side effects than with long prednisone courses in tablets. Metylprednisolone (methipred, Solemedrol, Urbazon) is most often used. This drug differs from prednisolone by the presence of a methyl group, which improves its binding to the corresponding receptors and provides a faster and active effect of methipred on target cells. Metipred reduces the permeability of the vascular wall, normalizes the function of the BGB, reduces the swelling, has a small desensitizing and immunosuppressive effect. The drug is able to penetrate the BGB, therefore it has both a common and local anti-inflammatory and anti-ethnic effect, as evidenced by a decrease in the number of foci of demyelinization, accumulating contrast, with an MRI study. Side effects - lymphopenia, monocytopenia, an increase in blood glucose and transient glucosuria, electrolyte disorders, activation of fungal diseases, dyspepsia, abdominal pain, sleep disorders, a decrease in body weight. As a rule, a short rate is 500-1000 mg per day (at 400-500 ml of isotonic sodium chloride solution) for 3-7 days, depending on the severity of the exacerbation and severity of immunological signs of activation of the disease. After that, it is possible to carry out a short supporting course of prednisolone in tablets, starting from 10-20 mg every other day and reducing the dose of 5 mg. Clinical improvement occurs more often after 2-3 doses. Contraindications are peptic ulcer of the stomach and duodenum, sepsis and sideflines From the use of methipred in history. In the malignant course of the disease, the combined use of corticosteroids with plasmapherester or with cytostatis, but the latter is rarely used, since the risk of summing side effects is increased.
In the absence of methipred, you can use dexamethasone. Its clinical, immunological and side effects are close to such methipred. Dosage: 8 mg 2 times a day, reducing 2 mg every 2 days. The main problems using dexamethasone are associated with more pronounced than methylprednisolone, inhibition of their own corticosteroid products. If the exacerbation of the PC is manifested by isolated retrobulbar neuritis, sometimes it is enough to administer dexamethasone retrobulbarly to 1 ml for 7-10 days.
In the absence of listed drugs, it is allowed to carry out a prednisolone course in tablets (1.0-1.5 mg per 1 kg of body weight every other day, 2/3 doses in the morning, the rest of the day, for 15-20 days, then gradually reducing the dose of 5 -10 mg every 2-3 days with full cancellation per month). This course is significantly less effective than the introduction of methylprednisolone. When using long prednisiolon courses, in addition to the pronounced secondary immunodeficiency, the delicate of adrenal corthes and Izeno-Cushing syndrome, osteoporosis, a stomach ulcers can be observed lymphopianic, monocytopenia, increasing blood glucose levels, transient glucosuria and other severe adverse reactions.
Stimulants of production of endogenous corticosteroids, namely ACTH and its synthetic analogies (synacten-depot), are used in the bosting of the remitting form of PC and the increase in the activity of the disease under progressive forms. The main advantages of ACTH are a small amount of side effects, maintaining endogenous products of steroids. At the same time, some patients may experience swelling, changes arterial pressure, hypertrichosis. ACTH normalizes the permeability of the BBE, contributing to the decrease in edema, a decrease in cell content and cerebrospinal fluid IgGV. Improving the state of patients occurs, as a rule, during the first days after the start of treatment. The most common scheme: 40 UK ACTH intramuscularly 2 times a day for 2 weeks. The synthetic analogue of the ACTH is a synacten depot. The drug is most effective in patients with non-heavy damage to the central nervous system in the active stage. Recommended scheme: 3 ml intramuscularly 1 time per day 3 days in a row, then 3 ml intramuscularly 1 time every three days 3-7 times depending on the severity of exacerbation.
In the pathogenesis of exacerbation with PC, nonspecific reactions characteristic of any inflammatory process are essential. In this stage, the use of angioprotectors and antiagregants, strengthening the vascular wall and reduce the permeability of the BCB, is justified. It is recommended to use Cararentil courses (0.025 g 3 times a day per hour before meals), Trental (0.1 g 3 times a day), nutitin and glutamic acid (every drug 0.25 g 3 times a day). Antioxidants, such as alpha tocopherol, can be used to potentiate an antiagregating effect. These drugs, as well as inhibitors of proteolytic enzymes, in particular, trausilol, contrikal or mining (3-7 times intravenously 25,000-50,000 units in 500 ml of isotonic sodium chloride solution), Epsilon-aminocapronic acid (100 ml of 5% solution 5 -7 days once a day), they suppress some mechanisms of direct fabric damage under inflammation, in particular the action of proteolytic enzymes of macrophages and products of free radical reactions.
Currently, it is possible not only to introduce immunoactive drugs, but also to derive pathological agents from blood using plasmapheresis. During PC, the modulating effect of plasmapheresis may be associated with the elimination of the spree of myelin, antigens, antibodies, immunologically active substances. At the same time, an acute allergic reaction to the introduction of plasma can be observed, leading to the exacerbation of the PC, therefore it is often used frozen plasma or complex protein blood substitutes. During PC, the effect of plasmapheresis was investigated when the disease with the remitting current and in the chronically progressive course, in the latter case, often with the introduction of corticosteroids. The improvement in the exacerbation of the PC was noted in approximately half of the patients, more often with a non-heavy defeat of the central nervous system. The clinical effect was better with the duration of the disease under 3 years. At the same time, it should be borne in mind that some plasma components can perform a compensatory function and their removal is undesirable. Plasmapheresis is carried out once a week with a plasma exchange, which makes up 5% of the body weight. Course of treatment 4-10 sessions. A significant side effect, in addition to allergic reactions, is the removal of immunoglobulins from the blood, so sometimes the procedures are complemented by the introduction of intramuscularly serum immunoglobulin. The combination of plasmapheresis with corticosteroids sometimes reduces the dose of the latter. For the removal of pathogenic substances during the exacerbation of the RS, intravenous drip administration of hemodesa is possible (200-400 ml per day for 3-5 days). The risk of side effects at the same time is significantly less. In this case, there is sometimes a quick favorable clinical effect, which involves a possible anti-inflammatory effect. Thus, with the exacerbation of PC drugs, methylprednisolone and ACTH are, in some cases, they can be combined with plasmapheresis, antiagregants, antioxidants and preparations that strengthen the vascular wall.
With a slowly progressive course of the disease, for example, with a secondary progressive course, the appointment of strong immunosuppressors is inappropriate. In these cases, the use of metabolic preparations, complex symptomatic and rehabilitation treatment is more substantiated. Positive effect Sometimes they give repeated courses of ACTT drugs (with good tolerability), which do not cause depletion of adrenal cortex and other delayed side effects. In the primary and secondary progressive course of PC, repeated courses of synctena-depot of 15-20 injections are possible. With malignant, steadily progressive variants of the PC flow are used strong immunosuppressors. Among the drugs of cytostatic and antiproliferative action, Azatioprine, cyclophosphamide, cyclosporine A, Claderybin, Methotrexate, and general irradiation of lymphocytes were investigated. As a rule, these drugs are prescribed with a malignant, steadily progressive course of the PC and the ineffectiveness of recreational corticosteroid courses. In some countries, in some cases, anosatioprine is used (at a dose of 1.5 to 3 mg / kg of body weight with a possible increase in dose of 25 mg each month, the course is stopped with a decrease in the number of leukocytes in the blood to 4 x 10 ^ 9 / l), less often cyclophosphamide. Among the side effects most frequent and severe are the suppression of the bone marrow function with leukopenia and anemia, disorders of the liver functions and gastrointestinal tract. Less side effects gives cyclosporine A, which provides selective effect only on activated cells carrying receptors to interleukin-2 (IL2). The appointment of this drug should be carried out strictly individually and in the extremely chicken firing cl teaching x with a rapid increase in neurological deficit. The most convenient and least toxic form is the preparation of Sandimmun, taken inside 3.5 mg per 1 kg of body weight 2 weeks, then 5 mg / kg for another 30 days. Supporting courses are possible. Side effects of Sandimmuna are associated with nephrotoxicity of large doses of the drug, which is observed extremely rarely.
In the presence of secondary immunodeficiency in the subacute stage, immunomodulators with preferably helper action can be effective, of which the drugs of thymus (T-activin, Timalin, Timopentin, etc.) can be effective. T-activin is prescribed 1 ml subcutaneously 5 days in a row 1 time per day, then after a 7-day break in a row 2 injections subcutaneously 1 ml per day.
After receiving data on reduced products with the PC of interferons, carrying out the first protective reactions against viruses, numerous tests of interferon and their inductors began. Reliable scientific fact These are evidence that the introduction of gamma-interferon in a pure form and in the composition of crude preparations in interferon leads to the activation of PC, more often in the form of exacerbation. This is due to increased antigen-representing activity of macrophages, overall activation of immunity. Alpha and beta interferons in their immunomodulatory properties are antagonists of Gamma Interferon. These interferons are mainly antiviral exposure, reduce the products of activation cytokines and the activity of antigen-representing cells. Recently completed several studies of beta interferon: beta interferon-1b \u200b\u200b(Betaferon) and beta interferon-1a (rebiff and avonex) using placebo and double-blind method. These tests have shown that compared with a group of patients receiving placebo, against the background of a long permanent reception of beta-interferonov, the number of disease exacerbations (by 30%) is decreased, less new foci of demyelinization (according to MRI studies) is formed. The effectiveness of beta-interferon is marked with the remitting form of the RS under non-heavy lesion, there are preliminary data on its effectiveness and with the secondary progressive course of the disease. The sirogue use of these drugs is complicated by their high cost, the presence of small side effects in the form of local reactions to intradermal administration, fever, depression (to a greater degree of beta interferon-1b). The severity of systemic side effects is reduced by simultaneously use of pentoxyfalline (1600 mg per day) or paracetamol (600-1000 mg per day). Recently, studies are carried out to clarify the indications and diagrams of administration, a decrease in the cost of the course. It should be emphasized that beta interferon courses are preferably prophylactic in nature, i.e. Do not restore the functions disturbed by the preceding exacerbations of the disease. Therefore, the drug is most effective in the early stages of the PC, with a non-heavy defeat of the CNS. Against the background of the beta-interferon course, the RS exacerbations are possible, in which corticosteroids or ACTH drugs are also prescribed. The optimal duration of the treatment rate of beta interferon is still unclear. The course of treatment should be discontinued in the presence of pronounced side effects or with the ineffectiveness of treatment in this particular patient (if there are three RS exacerbations throughout the year or the rapid progression of the disease). Alpha Interferon tests also gave first encouraging results, but this drug has a large number of both local and general side effects.
Copaxone's clinical trials (CPA-1, Copolimer-1) are completed with the remitting forms of PC. Copaxon is a synthetic polymer of four amino acids: L-alanine, L-glutamine, L-lysine and L-tyrosine. Its formation occurs during random polymerization, the molecular weight ranges from 14 to 23 kDa. It is assumed that peptides similar in structure with the main protein of myelin cause the induction of tolerance, a decrease in the products of activation cytokines. Conducting a long-term course of Copaxon also leads to a decrease in the frequency of RS exacerbations. Studies are conducted on the use of other peptides and amino acids, antioxidant.
Currently, clinical trials of the method of induction of tolerance to various myelin antigens are carried out by taking other peptide analogues. Perspective studies on the directional modulation of cytokine products, the introduction of large doses of immunoglobulin intravenously, methods of selective immunocorrection. The preparations of peptide nature, which have a distinct regulatory influence on both immune and nervous system, i.e. affecting the state of the "neuroimmune network". A selective approach to the stadium treatment of PC is developed based on and under the control of data of clinical and immunological research.
Symptomatic therapy. This section of the RS therapy is currently paying increasing attention, especially when stabilizing the disease. Symptomatic therapy is carried out in close connection with the medical and social rehabilitation of patients and in many cases has a great influence on the state of the patient PC and for the course of the disease. An important aspect of the symptomatic therapy of the PC is to reduce the pathological muscle tone. For this purpose, Miorolaksanta (Sirdalud, Baclofen, Middokalm) are prescribed, benzodiazepine-type preparations (diazepams, vigaboline, dancen), igloreflexotherapy, point massage, apply physical relaxation methods. The dose of drugs is selected individually, and gradually increases with small to optimal, in which there is a decrease in spasticity, but weakness in the limbs does not grow. The new potent method is the injection of botulin-toxin, blocking the synaptic transmission in peripheral nerves. This method is expensive, requires caution and special skills, but is the strongest means effective even with the development of spastic contractures.
In some cases, with a moderate increase in muscle tone, especially in the spinal shapes of PC, hyperbaric oxygenation sessions (HBO) are effective. In some cases, HBO courses contribute to a decrease in the severity of violations of the functions of the pelvic organs. Violations of the functions of pelvic organs, including sexual disorders, can also be adjusted by magnetostimulation. In terms of delivery hyperexia, anticholinergic preparations are used, tricyclic antidepressants. A large problem for patients with the lower parapapene represents frequent imperative urges and urinary incontinence in day and night. In these cases, the preparation of choice is the desmopressin (an analogue of vasopressin), effectively reduced urine products at a dose of 20 μg. An important point in the treatment of disorders of the functions of pelvic organs is prevention of urinfections. In some cases, periodic catheterization is needed for complete release of the bubble, since any violation of the passage of urine stimulate development infectious diseases. Apartments are prescribed: 5-nct or nitrofuran derivatives (Furazolidon, Frazolin, Furadonin). To correct the dysfunction of the vegetative nervous system, vegetotropic agents are prescribed, with dizziness - betaner or stamp, according to testimony - psychotropic drugs. A serious problem is treatment with coordination violations and intentional tremor. The severity of these violations can be reduced by assigning vitamin B6 courses, beta-adrenoblasts in combination with tricyclic antidepressants. To burn a pronounced tremor reaching the degree of hyperkinesis, carbamazepine (Finlepsin, Tegretol) can be used with a gradual increase in dose from 0.1 to 1.2 g. In some cases, with moderate manifestations of ataxia, the amino acids are effective, in particular glycine. Symptomatic means include metabolic therapy that promotes regeneration of affected tissue and maintaining a balance in immunoregulation. Metabolic therapy courses are carried out by PC patients once every 4-6 months (cerebrolysine, essential, glycine, nootropyl, cerebral, encefabol, group vitamins, vitamins E and C, methionine, glutamic acid). Showing the leaf, massage (with low muscular tone). In heavy patients with hypotrophy, it is possible to carry out courses of treatment with anabolic steroids, such as retabilic.
Prevention of sclerosis dispelment
Patients of the PC should avoid infections, intoxication, overwork. With the appearance of signs of a general infection, compliance with the beddown is necessary, the appointment of antibacterial drugs, desensitizing agents. It is advisable to limit thermal procedures, hyperinsolation is contraindicated. At the RS, it is recommended to maintain maximum activity in all areas of vital activity, if this activity is consistent with the capabilities of the patient and excludes frequent overwork. The PC patient should participate as much as possible in the life of society, and insulation adversely affects the course of the disease, especially on the frequency of its complications. It is such changes in the methods of conducting patients, neuroability in combination with modern methods of pathogenetic and symptomatic treatment changed the clinical picture of the disease, and many patients have a favorable form of the course of the disease with long-term remissions.
The Ministry of Health of the Russian Federation approved the drug revalide (Elrombopag) to use in children. The new drug is shown by patients with suffering chronic immune thrombocytopenia (idiopathic thrombocytopenic purple, ITP), a rare disease of the blood system.
03.03.2017
Canadian scientists from University in Ottawa intend to revolution in rehabilitation medicine. In one of the last experiments, they managed to grow a human ear from an ordinary apple.
27.02.2017
Specialists of the First Medical University named after Pavlov in St. Petersburg created nanoparticles with the help of which the diagnosis of infarction and pre-infarction states of the patient is possible. Also in perspective of research, nanoparticles will be applied ...
Medical articles
Viruses are not only twisted in the air, but also can fall on handrails, seats and other surfaces, while maintaining their activity. Therefore, on trips or public places it is desirable not only to exclude communication with the surrounding people, but also to avoid ...
Return good eyesight and forever spread with glasses and contact lenses - the dream of many people. Now it can be done by reality quickly and safely. New possibilities of laser correction of vision opens a completely non-contact technique of Femto Lasik.
Cosmetic preparations designed to care for our skin and hair can actually be not so secure as we think
Lactostasis is a condition due to a delay breast milk in the gland and its ducts. With one degree of degree of severity of lactostasis, every woman in the postpartum period is found, especially if the birth was the first.